




Rediscovering Biology: Molecular to Global Perspectives
Emerging Infectious Diseases Expert Interview Transcript: Judith M. Martin, M.D.
 Pediatric Infectious Disease
Pediatric Infectious Disease
Interview Transcript
Tell me about the longitudinal study that you are conducting here, and how that started.
I was starting off as a faculty member here, and I needed a project. So my mentor was very interested in respiratory infections. So we said, “what niche hasn’t really been filled yet?” So we thought about doing strep infections in children, because we had a lot of questions. You know, why do some kids get repeat infections after each other, and other kids get no infections at all. So we thought about doing a longitudinal study at a school, where we could follow kids over time and see what happens, to see if we could answer some of those questions.
Would you define longitudinal study? What does that mean?
A longitudinal study is one where you follow a group of children over time, and so it’s not just a one-time visit, “do you have strep or not? Goodbye.” You have a long relationship with them, as we’ve had with many of these kids, we’ve seen them now for five years. So it’s a pretty long time to follow them serially.
When you started this research, did you expect to find any surprises?
Well, we knew that this was really groundbreaking in that nothing like this had been done, and in this era where we have all these molecular tools and things that weren’t available 20 years ago to really look at the different strep infections we’ve seen. To say, you know, how many different kinds are in the community at one time, and does that change from year to year? So we knew we had all these questions that had not previously been asked, because the tools weren’t available to ask them. That is very cumbersome and time-consuming to do a longitudinal study like this. So no one else has ever done it over time. So we knew it was groundbreaking, and that it hadn’t been done before with these tools. So certainly we were going to come upon a lot of information that wasn’t previously known. We didn’t know what to expect, but we thought we would be able to make a pretty big contribution.
What age group of kids did you use, and why did you pick that age group?
Strep throat really affects kids between the ages of 5 and 15. After that, you don’t get as many strep infections, and so it’s not in the high school-age kids. So we wanted to target a group of elementary school children since they are really the primary population that gets strep infections. So the kids that we studied were between kindergarten and 8th grade.
Which bacteria is the culprit here with strep infections?
So we’re talking about Group A streptococcus; another name for it is Streptococcus pyoganes. It’s the bacterium that causes strep throat infections in children. So those are commonly infections where the kids will have a prominent sore throat. They might have headache, fever. Some kids have a belly pain with it. But it is a pretty frequent infection in school-age children.
What are some other ranges of diseases that strep causes?
It causes pharyngitis, or sore throat. But it can also cause invasive infections. So that is when the bacteria actually get into the blood stream. It can cause a blood-borne infection, bacteremia or sepsis syndrome. It can also cause pneumonia, sinus infections, and there are a lot of skin infections, from a simple cellulitus, which is just a soft tissue infection, to the one that we hear about, the flesh-eating bacteria. That is usually caused by Group A streptococcus.
But we all harbor these bacteria don’t we? Why does it cause disease in some and not in others?
That’s a big question we had. We know that it’s ubiquitous. It’s everywhere, and many people have it as just one of the bacteria in their throat, and it’s not causing them any problem. No one really knows how immunity develops to the bacteria. That is probably what protects us for the most part from getting infections with it. It probably happens over time. That is why children are the ones who get strep throat and not adults, for the most part, because they haven’t been exposed to it.
Kids are more likely to get strep infections than older people, and it is because there are many different types of strep. It’s felt that when you get exposed to different types over time, you develop some sort of immunity to those infections. So by the time you’re an adult, you see many different types of strep and are now protected from them. So kids are more likely to get strep infections because they are naive. They haven’t seen the streps, they get exposed to them, and they get sick with them. But over time, they are able to fight off those infections. Now you still hear about adults getting strep throat, or even the more serious infections, the invasive infections. It’s likely that happens because they don’t have immunity to that particular strain of strep. There are over a hundred different types of Group A strep. So they may have seen over 50 of those in a lifetime. So if they happen to get exposed to the one they haven’t seen, they could still get sick with it.
Tell me what happened during the first year of the study.
So the first year of the study was really, you know, we were trying to figure out, was this going to work? Would kids really tolerate this number of throat cultures over time? Would we tolerate doing the work? How would we know about enough strep infections? So that was really just a pilot study to see, could we do this? We found out it was feasible and the kids were great, and they really tolerated the throat cultures. So we realized we could go on and do more. So the first year of the study we just studied 48 children. The second year of the study, we were lucky enough to get 75. Then the third year of the study, we had 100 children. So we were able to follow those over time. Really the first year we were just looking at what the patterns were for infections. How often did kids get sick? Was it more common or less common than we thought it was going to be? So nothing too dramatic in the first years, pretty much what we expected. We had a lot more children who just carried the bacteria in their throat than we expected. Again, nothing like this had been done before, and so we weren’t sure where the numbers were going to fall. So that was our most remarkable finding in the first year of the study.
All you do is put a little swab in the throat to take a culture, is that right?
Yeah, it’s not a complicated study. We are really just collecting throat cultures over time. It’s the time that is the time-consuming part. Every two weeks, these children will get their throat cultures performed, and then we go back to the lab and process the throat cultures.
In the third year you started getting some interesting results. What happened?
The first couple years we were just looking at patterns of infection. But all along, we were testing the sensitivity of the antibiotics, meaning we would take the Group A strep and test to see that if the different antibiotics that were supposed to work, would work. So the first year of the study, all of the Group A streps that we found were sensitive to Erythromycin and Clindamycin. In the second year of study, we saw the same thing. This was pretty much what we expected, because in the United States we knew that it is only about 2 to 3% of Group A strep isolates that are resistant. So we were just going along doing them, and then all of a sudden, halfway through the third year of the study, we started to see isolates that were resistant to the macrolide antibiotics. Once we started seeing it, it snowballed. It was almost half of the isolates from that year were actually resistant to the Erythromycin or macrolide antibiotics.
Define macrolide antibiotics.
So halfway through the third year of the study, we saw our first isolate that was resistant to Erythromycin. Erythromycin is one of the macrolide antibiotics, so it’s in a class of antibiotics that includes Erythromycin, Azithromycin, and Clarithromycin. They are the ones most commonly used here in the United States. So once we saw the first isolate that was resistant, it kind of snowballed, and almost half of the isolates from that school year were resistant to that whole class of antibiotics, the macrolides.
What was the percentage of resistant cultures you started to find?
There are 315 cultures from that year that are positive for Group A strep. Of those, half of them, it was 48%, were positive for resistance.
That is surprising isn’t it?
It’s very surprising; as I said, in the United States only two to three percent of the isolates were previously known to be resistant to the macrolides. So now, to have this great number, the question was, how did this happen? Was it just one strain that got in? This is probably the explanation, is we have this whole group of children who see multiple different types of strep over the years. And now we had a strain of strep that they hadn’t seen previously. We know from our first two years of the study that none of the children had had this strain before. So it wasn’t resistant, but it also wasn’t this M type.
When we talk about there being over a hundred different types of strep, we call them M types, or EMM types. So this specific strain that was resistant was an EMM 6, and we know there are very few EMM 6 isolates in the first two years of the study. So what that tells me is that it wasn’t in the community. The kids hadn’t seen EMM 6 Group A strep before, and so as a whole, the population didn’t have any immunity to EMM 6. So once the EMM 6 isolate got into the school, the kids were susceptible. They hadn’t seen it before. Many kids were able to get sick with that strain because they had no immunity. It just so happened that that particular strain was a resistance strain. So that is why almost half of our isolates were accounted for by this resistant strain.
And where did this resistant strain come from?
We know they are out there in the United States, but in smaller numbers. So it could have come from anywhere. I mean we don’t study the entire school. It may have existed in lower numbers prior to us finding it. But we have a pretty good percentage of the school. So I suspect, from the rapidity of the spread that we saw happen after we saw the first isolate, that makes me think that it wasn’t there before. It got into the school, and then every kid that was susceptible to it got it. But you know, many people travel. It’s very, very common in countries in Europe. So it wouldn’t be surprising.
So it’s not clear at all where it came from. It could have come from anywhere in the United States and just existed in small numbers. Then once it got into a population where the kids hadn’t seen it before, it was able to spread very quickly, because there was no immunity. But we know that these strains exist in small numbers in the United States. But they are very common in the European countries and other Asian countries like China and Japan. Nowadays, with travel being so easy, people travel back and forth, they have visitors form European countries, and they can bring the resistant isolates.
What is exacerbating this problem of spread?
So the antibiotic resistance is thought to be directly related to antibiotic use. We don’t, we can’t say, in an individual child, oh this child got x, y and z antibiotics, so they got the resistant strain. It’s more likely a community-wide problem. It’s been shown in countries in Europe such as Finland that when their antibiotic use of the macrolides increases, they see a corresponding increase in resistance to the macrolide antibiotics, and the Group A strep. When they identified this problem in the past, what they did was they made some interventions nationwide to decrease macrolide use. Once those interventions were put into place, they also saw a corresponding decrease then in macrolide resistance and Group A strep. So the two probably go pretty closely hand-in-hand. That’s the community-wide antibiotic use that we attribute to the bacteria becoming resistant.
How has the use of Azithromycin contributed to antibiotic resistance?
I think many drugs are used pretty commonly. Azithromycin has a lot of things to its advantage. It’s very convenient. It’s taken once a day for five days, as opposed to penicillin, which is taken once or twice a day for 10 whole days. So given a choice, many people would absolutely prefer to take a once-a-day medication for five days. So I think that has contributed a lot to its increased use in the United States. We know that antibiotic use is high in the United States. But we’ve also specifically tracked Azithromycin, and we know that use has increased over time. So it goes to show that it’s safe to assume that when any antibiotic, or any antibiotic class is increased in its use, you might see a corresponding increase in resistance develop to that antibiotic.
Is it being over-prescribed?
I think it is, because many people, as I said, given a choice, will chose to have something that is easier to take rather than something that is more complex. And especially with working parents, or single parents. If they only have to remember it once a day, it’s a lot simpler. So because of that convenience, many people would prefer that as opposed to some other medications.
Was that the first time in the US that the bacteria showed resistance to this class of drugs?
Well, there was a study that shows this 2 to 3% resistance when they looked at all the Group A isolates, and this was in 1997. It was 2 to 3% of Group A streps were resistant to the macrolides. So we’ve seen it before in the United States in low numbers. This is the first time it is seen in this high of a number in the United States. Now in some sense, it’s not really fair, because most people don’t do sensitivity testing for throat cultures. People get the rapid strep test. So there is no actual culture to have the bacteria to go on and test. It may exist in higher numbers in other locations-the tests just aren’t being done to get those results.
So even though doctors should really be doing those kinds of tests before they prescribe a drug, how are they going to have time to do that?
Most of the time, people can make a diagnosis using a rapid strep test. That’s fine if someone has classic symptoms of strep throat and a rapid strep test can be done to get your answer. Then you can get more appropriate use of antibiotics. Someone has strep throat; you give him or her the antibiotic. So that’s the nice thing about the rapid strep test. The disadvantage to them is then you don’t have those bacteria to go on and test for the antibiotic susceptibilities.
So knowing that the United States has had a low rate of macrolide resistance, we’ve never felt forced to push the issue and to do more testing. So I think now that we are seeing these pockets, at least, of increased resistance, that it doesn’t necessarily have to be done on a wide-scale basis. But we should at least look nation-wide to see if there are other areas that have increased resistance.
When resistance starts showing up in kids like this in little pockets, it doesn’t stay with the kid. Does it quickly move out into the community?
Well, kids are really the reservoir for the infections, because they are the ones that are more likely to be positive for the strep. So they carry the bacteria. So they are going to spread it to anyone else in the community that is susceptible. So if an adult, or their parents, are susceptible to that bacteria that they have never seen before, and don’t have immunity, they are likely to get infected with it. If they have seen it before, then they won’t get an infection with it. But that’s really how it spreads through the masses, if you will.
How quickly? When this first showed up in the school, how did you follow up on that in the community?
So we knew it was in the school, and it was entirely possible that the problem was just in the school and not in the greater Pittsburgh area. So we wanted to look at that issue. What we did is take throat cultures done on children that presented to the children’s hospital emergency department. We took those throat cultures and tested them for antibiotic susceptibilities. And we looked to see, was it elsewhere in Pittsburgh, or just in the school? What we found was that 38% of the isolates from the community that we tested were also resistant. So that really told us that it wasn’t just something that was isolated in the school that we were studying, but it was really in the whole community.
So it’s in the community of Pittsburgh. That had to be surprising to you, right? What are the ramifications of that?
Well, see, that’s why there is no reason to believe that Pittsburgh is different than any other major city in the United States. So that really prompted us to say, “we really do need to look at these other cities to see if they have the same rates of macrolide resistance.” So we’ve gotten together with 9 other centers in the United States. We are starting a project this fall where we are going to look at their throat isolates and do susceptibility testing on them also.
Do you have results from around the rest of the country?
Not yet, because really strep season is from November through May. So we really have just started it in the past two weeks. So we don’t have any results yet.
Would you characterize this study that you’ve done as a wake up call to the rest of the country?
I think it is, because we’ve been really been lulled into the sense of security that Group A strep in the United States were not resistant. So we didn’t need to worry about it. We didn’t need to test the bacteria, and we could just treat them, you know, with either penicillin or the macrolide antibiotics.
So the fact that we found this, and in this dramatic number, was really a wake up call. You know, hey macrolide resistance is here, it’s here now, and you need to consider that when you are treating a patient. Our recommendation is to go back to using penicillin. It’s a safe drug, it is an inexpensive drug, and it’s the one that is recommended for treatment of strep throat. Now there are going to be some individuals who are allergic to penicillin, and for those you’ll need to find an alternative. Often, you can use Clindamycin, which is a different medication that can be used to treat strep throat. If you’re really up against a wall, you can have the specific testing done for the patient that you are seeing to find out if you could use a macrolide antibiotic.
There are strains that still are susceptible or sensitive to the macrolide drugs?
We are lucky with this particular strain that it is still susceptible to Clindamycin. So we know that is another option for practitioners who need to treat a child who is allergic to penicillin and they have a macrolide-resistant strain. There are some strains than neither the macrolide antibiotics or Clindamycin would be effective against. But this is not the case in this situation.
When you say Clindamycin, is that different from Erythromycin?
Yeah, Clindamycin ends the same as Erythromycin, but it’s not in the same class of medicines. So it’s entirely separate, and it’s safe to use. For the strains that are Erythromycin-resistant, you can’t use Erythromycin, Azithromycin or Clindamycin. But you can always use penicillin. I mean that is the lucky thing with Group A strep. It’s smarter than we are, but it can not ever become resistant to penicillin. So it’s nice compared to some other bacteria that can become resistant to everything. It can’t ever become resistant to penicillin. If they try to make it resistant in the lab, it kills itself. So it’ll never be resistant. So we at least have one medication.
That is amazing. It seems that the bacteria would become resistant to any drug at some point.
Right, but it won’t, because the adaptation that it would have to make to become resistant has to do with the cell wall of the bacteria. If it makes that change, then it self-destructs.
So there seems to be a whole ecology that determines whether bacteria can get out into the environment and spread as disease.
Right, I mean it has to be just the right conditions, because you really have to be sick with the bacteria in order to effectively spread the bacteria. If you just have strep as one of the bacteria in your throat, but aren’t sick with it, then you’re not an effective transmitter of the bacteria. But if you’re sick with it, then you’re coughing, sneezing, and wiping your nose. You have it on your hands, and then you can spread it easily to another person. But if you’re well and you’re not having a lot of hand to face activity, then you’re not going to be able to transmit it.
So if there is a strain that becomes resistant, is there something you can do to try and alleviate that or to keep the resistance from spreading, by treating it with the correct drugs?
Well, as we saw in Finland, when they made nation-wide interventions to decrease macrolide use, they were very effective in decreasing the amount of resistant bacteria in their community. So we still have hope for these nation-wide efforts that we are making with the CDC and other organizations to really have appropriate antibiotic use. Then we can make these interventions, so we can hopefully also decrease the resistance that we see in the United States.
What is happening in this community in terms of going back to using penicillin?
Here, we know that it is here, and we know that it’s a problem, and so we’ve been very effective in teaching the physicians that are in our area, don’t use the macrolide antibiotics as your first choice for kids with strep throat. Go back to the penicillins, and for the kids that are allergic, use other alternatives, but really avoid the macrolides.
So they’re actually doing that?
Yeah, the physicians that I’ve spoken with have said that, because of what you found, we’re not using those drugs.
What is going on with this study now?
So it was year three that we saw that 48% of our isolates were resistant to Erythromycin. In year four, it was 52% of our isolates. So it was still there, and we’ve just begun year five of the study. We are still seeing the resistant isolates. So we know it’s still here in the community. We have seen fewer acute strep infections with the resistant isolate.
What is happening here in Pittsburgh with the virulence of this strain?
Well, we’re still seeing a lot of isolates that are resistant to the macrolide antibiotics. So it’s just as prevalent as it was in the third year of the study. But in terms of the virulence, it’s really less, because in the third year of the study many children got sick with this isolate. In the fourth year of the study, kids still got sick with strep, but they were with different strains of strep that were not resistant. So although the isolate is still in the community, it wasn’t really being transmitted as effectively as it was the year before.
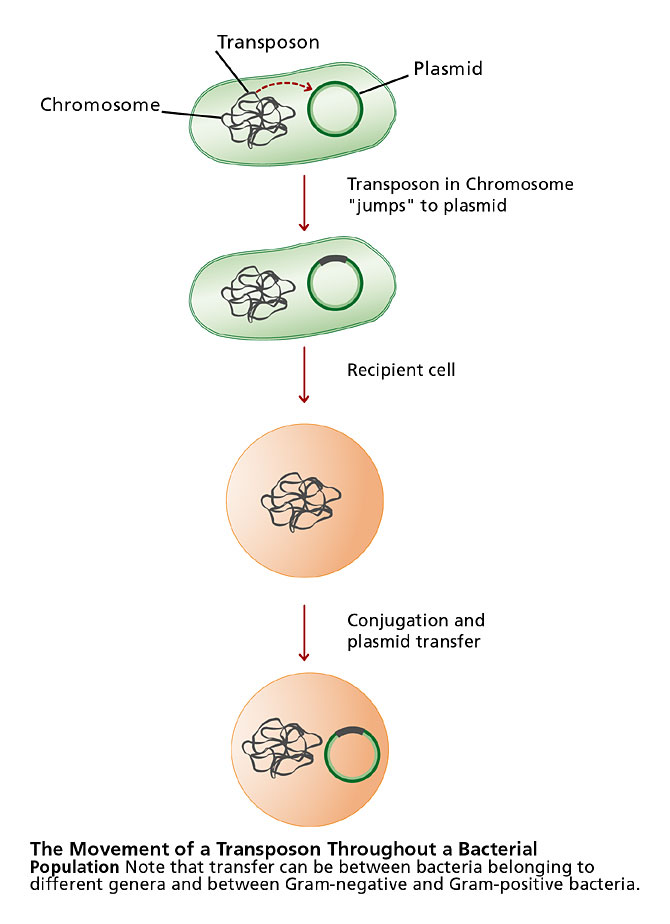
So can strains other than Group A strep develop resistance to these drugs?
There are a lot of intricacies about how the resistance spreads. Can the resistance spread from bacteria to bacteria without spreading from person to person? That is possible. So if I have two different types of Group A strep in my throat, and the one is resistant and the other isn’t. The resistant one can make the other one resistant also, and then I could spread that one. Certainly it’s a possibility, and it’s something that we need to keep looking at, and we’re following the students to see if that happens.
So it sounds like the bacteria are winning this war? What else can we do to combat the problem?
I think one way is just to be aware of the problem, and get back to avoiding antibiotics when they are not necessary. We know nation-wide that people are getting antibiotics for simple colds. And in adults and kids, many people have sore throats. Only about 10% of those people will actually have Group A strep as the cause of their sore throat. That is really the only cause of a sore throat that needs an antibiotic. So in one study that was done recently, 75% of people were walking away with an antibiotic prescription when only 10% of them probably really needed it. So it’s those places that we need to start making in-roads to decreasing antibiotic use. Luckily with strep you can make a diagnosis by doing a simple test. So it’s not a matter of do they have it, do they not? You can do the test to find out. Then, anyone who has strep, you can treat them appropriately with the antibiotics.
But the doctors are being pressured to prescribe something, and they’re giving in, then part of the problem is the health care providers’ society as well, isn’t it?
Absolutely, I mean it’s a lot easier to write a prescription than it is to talk to a patient, and to tell them, you know this is a simple cold. This isn’t something you necessarily need an antibiotic for. Let’s just take our time and watch what happens, and it tomorrow you’re son is sick again; we can look at him again and re-evaluate it. It’s a lot more difficult to have that conversation and to have the ongoing dialogue-to check in again the next day make sure that he’s not worse-than it is just to write the prescription and hand it to them so they walk out the door.
So what should doctors be doing-more testing on kids, or…?
I think it only needs to be done if they are in an area where you think that it exists and if someone is allergic to penicillin. I mean we still want people who are susceptible to be treated. We also still want physicians to go back to using penicillin or amoxicillin for kids who are not allergic to those medications. Because they are narrow-spectrum, they only kill the strep. They are inexpensive, and they are pretty convenient and safe, and they won’t cause resistance in the bacteria.
What are some of the unanswered questions that you are still looking at?
We are very interested in how children develop immunity to infections, because that’s not known. We just assume that it happens over time, but is it cross-type specific-so if I get exposed to types six, seven and eight, will I only have protection against six, seven and eight, or will I also get protection against types 15, 21, and 62? Certainly if there were ways to know that information, or to help develop more vaccines for things like Group A strep, then we could protect people in those ways.
That way, we wouldn’t be dealing with the issue as much with antibiotic resistance, because we could protect people from getting the infections in the first place. I’m certainly more drug development is going to help. But I guess it’s kind of like just a patch on the problem, because every time a new antibiotic comes on line, initially it is very effective for whichever bacteria it’s targeting. But as its use increases, it becomes less effective over time. Drug development will at least always work as a patch. Then the third thing that we really need to do is to instate more education, both of physicians and of families and patients, that antibiotics are not always the answer. That’s going to take a lot of time and a lot of changing in the way of everyone’s thinking, and making people more aware of this as an issue.
Was it really surprising how fast the resistance spread in the community?
It was very surprising, but kind of looking back now, from the information we have from the first years of the study…none of this was known before: What types were in the community? Does that switch from year to year? And what we’ve seen, at least in the school, is that each year there are two prominent M types for the Group A strep. They count for the majority of the infections. Then the next year, they are gone and there are two new types. So the fact that a new type would get into the school and cause infection in a large percentage of the kids, although it was surprising then, now in retrospect it isn’t that surprising, because that is the pattern we’ve seen each year. What is surprising was that it happened to be a resistant strain, because we didn’t know that resistant strains were that prevalent here in the United States. So that was really a slap in the face, which said, “Hey, this is here, it’s a big problem and we need to deal with this right now.”
So you found that 38% of the community bacteria were resistant?
Right, it was 38%. We tested the isolates of children that were seen in our emergency department, and 38% of those isolates were also resistant to the Erythromycin.
Are what are you doing with this information?
So a lot of the reason this study was started was to help figure out how we develop immunity over time. When we think about immunity, there are things in your blood that help protect you from getting an infection. So if the antibodies are there, then when you get exposed to something, your immune system goes and fights it, and prevents you from getting the infection. But there are also antibodies and things that protect us that are in our saliva. That’s where you’re first seeing the bacteria when you get exposed to it. Your saliva is really your first wall of defense. And what we’re looking at is to see if there are specific things in the saliva of kids who are recovering from strep infections that prevent them from getting the next strep infection. So we do a little experiment, where we have pharyngeal cells-those are the cells that are in your throat-we can grow them in a layer, and we can incubate that with Johnny’s strep that he got sick with, so we put those cells on top of that layer. Then we use Johnny’s spit, and then we put that in there, and we see how the strep sticks to the throat cells, to the pharyngeal cells. What we find over time is that, if we use the saliva from before the child got sick, there is nothing in the saliva to prevent the strep from sticking to the cells, so that is probably why they got sick. But three to four weeks after their infection, their saliva prevents that strep from sticking. So that is why they don’t get back-to-back infections with that same strep.
But some kids do get back-to-back infections. So they don’t have that critical something in their saliva?
Right, right that’s just it. So we don’t know exactly what it is in their saliva that is the critical factor, but we are doing those same experiments with kids who do get back-to-back infections. We find that their spit isn’t protecting them. So the next step is to take that saliva and do specific assays to see what is it in the spit that is protecting the child from getting another infection.
The kids seem to have a great time coming to see you. I know they don’t know what’s going on scientifically, but do they have a sense that they are doing something helpful?
They do, and I think that many of these kids-it’s a private school, and many of their parents are professors or physicians-so they have some appreciation of what research is, or at least that you’re studying something; you have a question and you are trying to find an answer. They know that they are part of this, trying to find an answer. More so in the older kids than the younger kids. But then with this publication last year, many of them knew of it at least-not that they read the New England Journal of Medicine, but they read the newspaper, or their parents showed them, or it was on the local news. So they knew that they were part of it. I think that really helps with their ownership of how they really made a difference. And the kids do love it. They are really a great group of kids. I couldn’t have done anything without them.
Why is it important for doctors to know what strain of Group A strep they are dealing with before they prescribe?
It’s important that the physicians know what strep are in the community, because they can tailor their practices accordingly. So if they know that there is a lot of macrolide resistance in the community they are practicing in, they can avoid the use of the macrolide antibiotics. Some communities may be blessed, and will not have that complication, and so then physicians would have a choice and could use either of those two antibiotics.
How long will this study go on?
It will go on for as long as we have money (laughs). No, this (2003) is supposed to be the last year of the study. There is another question that we are asking this year that is different, and so if we get that answer with this year’s data, then this will be the last year of the study. We have reams and reams of data and information to pore over, so we’ll be looking at the results of this study for several years after that. But I believe this will be the last year that we obtain the throat cultures from the children.
Do you thing they will probably miss you?
They will.
What is the big message about your research that you want to leave us with?
It’s just that we really thought that Group A strep were sensitive to all the antibiotics out there, and what we really found out that is that this is no longer the case here in the United States. Group A strep are resistant to the macrolide antibiotics, and we need to take that into account now when we are treating patients.