




Rediscovering Biology: Molecular to Global Perspectives
Emerging Infectious Diseases Expert Interview Transcript: Stuart B. Levy, M.D.
 Scientist, Environmental Defense
Scientist, Environmental Defense
Dr. Levy is a professor of Molecular and Microbiology and a professor of Medicine at Tufts University in Boston, Massachusetts where he researches the Tetracycline Efflux Protein. He is also the President of the Alliance for the Prudent Use of Antibiotics, which is an organization that aims to promote responsible and appropriate use of antibiotics around the world.
Expert Interview Transcript: Stuart B. Levy, M.D.
Dr. Levy is a professor of Molecular and Microbiology and a professor of Medicine at Tufts University in Boston, Massachusetts where he researches the Tetracycline Efflux Protein. He is also the President of the Alliance for the Prudent Use of Antibiotics, which is an organization that aims to promote responsible and appropriate use of antibiotics around the world.
Tell me a little about the Alliance for the Prudent Use of Antibiotics.
In 1981, I guess I got frustrated with seeing all this antibiotic resistance occurring in developing countries and not finding a conference or a way in which the developing country experts and the industrialized world were getting together. With two other individuals, I organized a conference in the Dominican Republic. It’s was probably the first such conference where people from all over the world were coming to meet on a subject of resistance, antibiotics, and the genetics; about the ways that bacteria exchange resistance traits. And from the meeting came a statement that said that there is a lot of resistance out there, and it’s coming from the overuse of antibiotics. And what emerged was a press conference on the subject, and a statement that said we ought to improve our use of antibiotics.
It got a lot of publicity. It got a full page in Nature, describing this as a real challenge, and asking scientists, “Do you really think you can meet that challenge?” And we decided to start an organization, and we called it the Alliance for Prudent Use of Antibiotics, because we realized that the situation was going to be not one country telling another what to do, but an alliance of different countries, towards a global solution to the problem.
That was in 1981, and we struggled, but we kept it going, with really a part-time secretary and myself, and some members to put out a newsletter and do as much publicity as we could. This was before the web, and it’s gotten a lot easier now.
Well so was this the first time that there was really a global focus on antibiotic resistance?
In fact there was more ignorance of the topic. There was a problem. It was individualized in a particular hospital. The strains were being studied in sophisticated laboratories, but they came from other countries. Everyone was amazed at how bacteria resisted drugs. But there was not a coordinated effort to improve education, public education, to make it a global issue. That’s what the Alliance did, and it was the first and I think still the only organization that looks at a therapeutic application, and not at a particular disease. We are not the Heart Association, Cancer Association, Huntington’s Chorea Association, or whatever. We are dealing with antibiotics, trying to improve and curtail their misuse. Because we saw that they were used in so many areas, of course worldwide, that they deserved their own organization in order to improve their use, hold them, maintain them, and curtail their misuse.
So you are looking to curtail their misuse, but are you also monitoring strains of resistant bacteria around the world?
Well we have grown considerably since our origins in 1981. We now have I think up to 15 people working in the organization. And we have organized different efforts to look at where resistant bacteria are. What kind of resistance do they have? We have two such efforts. One is recently funded through the National Institutes of Health. We call it ROAR, like a lion roaring. But it’s Reservoirs of Antibiotic Resistance. What we do here is look at bacteria that are not harmful-at least not to people. They could be in animals, they could be in plants, and they could be on your skin. We want to know what resistances they carry, because they could be the ones to transfer their resistance to bacteria that are harmful. So we’re getting a surveillance of resistances and not caring where they are, but focusing on those in disease- and non-disease-causing bacteria. A complement to that is a project that the APA has gotten off the ground that is a surveillance of the clinically relevant bacteria. This makes use of a number of worldwide surveillance systems funded through industry. In many respects, it’s to test their new drugs. The data they get on their new drug, they keep for themselves, but they have a lot of data on bacteria resistant to drugs that are out there made by other people, made by the companies and made by other institutions. We can use that data for public health purposes and be able to look at the level of resistance in different parts of the world. That global advisory, as we call it, an antibiotic resistance, is mounting in its perspective. That is, in the breadth and in the number of strains that is affected. We have hundreds of resistance sites that we’re looking at through our collaborators, which include Bristol-Meyers Squibb, GlaxoSmithKline, AstraZeneca and other groups. The World Health Organization (WHO) serves as an advisor. The Centers for Disease Control and Prevention (CDC) is an advisor. And we’re very pleased, because it was not easy to be able to join these groups together to be able to come up with a picture of the problem, and then also to look for trends. What is happening over time?
So you’ve got kind of a global watch now going on?
We have now a global watch on clinical isolates, that is, those that cause disease. And more recently, on bacteria that don’t cause disease.
We are talking about resistance, so tell me, what are resistance genes? How do bacteria get to be resistant?
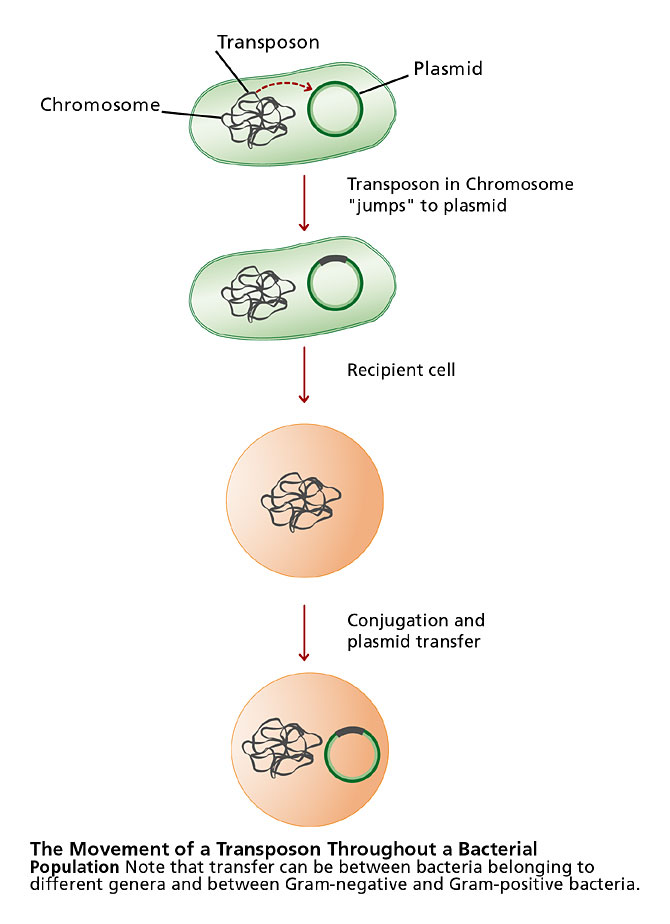
The bacterium has one chromosome, which is made of DNA, and it directs the synthesis of all the proteins it needs to survive, to grow, and to multiply. In addition, it can acquire other genes for lots of different traits. Among those are traits for antibiotic resistance. Now these genes, which encode or direct the synthesis of the traits or proteins that give you resistance, can come to the bacterium from lots of different sources-that is, other bacteria-by different means. They can be carried on small pieces of many chromosomes or plasmids, which can multiply by themselves. They carry with them a lot of genes for proteins required for them to multiply, but also to produce antibiotic resistance. They can come in on small pieces that we call transposons, which will jump from the plasmid to the chromosome or to another plasmid, and they carry resistance-they could carry many resistances-but they are called jumping genes. There are viruses that can do the same thing, can move resistance genes in and out. So there are lots of ways to acquire these resistance genes. Each of them codes for a mechanism to provide the bacterium with a resistance or an immunity to the antibiotic.
Are these resistance genes all carried on plasmids?
Resistance genes are carried in bacteria all over. In the soil, on your skin, in your intestinal tract, and most of them are in bacteria that cause no harm to you, but the genes can be picked up and transferred to those that could harm you. They can be borne on that single chromosome that a bacterium has, and they can jump from there or they can be released from there and go to another bacertium. They could be on these transferable pieces of DNA that we call plasmids. They can get in and out of a bacterium that way. They can come in with bacterial viruses. But out in nature, they are in a bacterium, somewhere.
How did bacteria get the first resistance gene? Once we developed antibiotics, did the resistance just kind of appear one day?
There is a lot of discussion as to the origin of antibiotic resistance genes. Probably the best argument is that they were intially protective to the bacteria that were making antibiotic substances in the first place. So if you’re a bacterium, and you’re making an antibiotic for whatever purpose-maybe as an antibiotic itself or as a byproduct of some unrelated biochemical process that you’re carrying out naturally-you don’t want to be killed by that. So you have a resistance mechanism built in. And somehow, that resistance gene or genes came out of you and moved to another bacterium that isn’t making the antibiotic, but now resists the antibiotic. Because these genes are transferable, and they eventually got transferred to other bacteria. In the process, mutations could occur, adaptations could occur. But the basic mechanism, in fact, we find in many of the producing organisms, it won’t be exactly the same structure, but the mechanism is the same. It’s an inactivating enzyme, it’s a pump that pumps things out. So the origin comes from bacteria themselves, and they probably were not made specifically for an antibiotic purpose. They could be dealing with other things. After all, bacteria have been around for millions and millions of years. You see, they saw dinosaurs come and go, so they’ve seen it all, and we, by using antibiotics, have sort of recruited out, from wherever they are, those resistance genes in the bacteria that now survive the treatment. Once we’ve got a population of bacteria that all have the resistance genes, that is a pretty good donor group that can then transfer those genes to others. Before you know it, we have the situation we’re in today, where antibiotic resistance is widespread, all over the world.
What are some of the other ways that bacteria can acquire resistance genes?
The earliest mechanism understood for resistance or for any change in the bacterium is by mutation. Spontaneously, once every hundred million times a bacterium multiplies, a mutation can creep into any particular thing it does or way that it moves. If it is a lethal mutation, they will die; if it isn’t, they will change. The Darwinian idea is that if they make that change and it helps them, then that change becomes more permanent. So a mutation to a gene that results in a resistance to an antibiotic like penicillin in certain bacteria could be a mutation in the target. And those bacteria survive, and their progeny now carry that mutation. There is also the chance that a mutation will change back, as we see in some of the finches in the Galapagos Islands, where, when the temperature changes and other changes occur, the species can go back another way, through mutations. But as long as the selection for that particular mutation is there, it will stay.
So you mean it’s basically survival of the fittest?
Yes, there’s no question about it. The best, simplest way to look at antibiotic resistance is that it is survival of the fittest. And it is evolution at a very rapid pace, because antibiotics are being used in such quantities that the rare mutations that might have never made it in normal times-now, if they give the bacterium the ability to resist an antibiotic, they are there and they are there to stay. So we’ve now created in a sense a new bacterium. We’re seeing evolution sped up like a film at high speed. And the consequence is devastating.
Could you define transformation?
Among the mechanisms by which bacteria can pick up DNA, or among the mechanisms by which bacteria can pick up antibiotic resistance genes, is by just incorporating naked pieces of DNA that are left behind when a cell dies or lyses, it breaks open. Not all bacteria can do this, but some can. The bacterium Haemophilus can do it. The bacterium pneumococcus can do it. They can pick up these pieces of DNA and incorporate them into their single chromosomes, and now they are resistant. The process is called transformation.
So dying bacteria just have to be in the same vicinity for a live bacterium to pick up their DNA in transformation?
Right, the DNA can just be present where a live bacterium is growing. I mean they can be multiplying, and there is a foreign piece of DNA there. They can pick that up and put it into their genome, and it could be only a small portion of that colony that is growing. But you throw an antibiotic on it, and you’ve destroyed all the others except for that one cell. Now it has all this room to grow, too. Suddenly you have a colony of nothing but resistant bacteria.
Could you explain a bit more about the specialization of some bacteria in transformation?
In order for transformation to work, that is for naked DNA to be picked up by a bacterium, it has to be seen and sensed by the bacterium. It’s got to have a receptor, we think, to hold onto the DNA. Then it’s got to be transported through the bacterial cell wall inside the bacterium. Then it has to have certain enzymes that can take that DNA and incorporate it into the genome, into the DNA of the chromosome. So there are multiple steps. In most, and in fact all instances known so far, transformation is fairly limited to bacteria of the same kind. You can understand that, because in order to get incorporated into the chromosome, you’ve got to find a site that is pretty familiar, and if you’re in different bacteria, it may not be. That’s why pieces of DNA like a plasmid or a transposon, which can just jump in and push its way into the DNA and get incorporated, work among bacteria of various different types, whereas transformation occurs only in bacteria of the same type.
So transposons can move between different kinds of bacteria. That’s a pretty interesting ability for a piece of DNA.
Yes, transposons are unique entities. We know they exist not only in bacteria, but in higher organisms as well. Corn, we know, for instance. Even in our own genomes. There are these jumping genes. These pieces of DNA that can jump out of one place and jump into another. They don’t need to be like anything in their vicinity. So we can see plasmids with transposons. We can see chromosomes with transposons. We can see bacterial viruses with transposons. And they are unique in being able to go from one piece of DNA to another. It doesn’t matter what its origin is. It could be between bacteria that are so different that they are evolutionarily as far apart as cats and dogs. Instances where we could never expect DNA to get incorporated, they do it.
Do we have any understanding of why they can do that?
No one really understands what causes transposons to move. We know enzymatically how it works. Why should they suddenly they move out of there, though? Perhaps something biochemically drops below a set threshold, and they are unstable and they leave. Something might come in and disrupt them, and they leave. But it’s going on all the time, of no consequence. Except when you’re acquiring a gene that you need, such as a resistance gene in the presence of an antibiotic that could kill you, then you survive.
Transposons have also been described as a sort of wrangler; they can bring multiple resistance genes into a single plasmid. How do they do that?
There are transposons that carry one, two, or more antibiotic resistance with them. There are other kinds of transposons that are called intergrons. Now the intergron I liken to a Venus flytrap. They’re waiting there for a resistance gene to come along like a fly, and then they clamp on to it and they incorporate it. I mean, the Venus flytrap will eat it up. What the intergron does is put the new DNA into itself and then look for the next one. So you can have 8, 9, 19 different resistances all lined up in this one unit, which itself can move. But it’s a specialized way to accumulate resistance genes.
Are these multiple genes for resistance against different types of antibiotics?
Each of these genes is for resistance to a different antibiotic. That is how we now understand the multi-drug resistance that we see today. The bacteria either acquire separate transposons or transposons that have 1, 2, or 3 genes, or these large composites of intergrons that could have large numbers of different resistances all accumulated in this one spot-integrated and run by this single genetic machinery.
How pervasive is this, and how big of a problem is this in terms of human health?
The fact that genes for resistance can move between bacteria of different types makes the problem of resistance that much greater. Instead of having that resistance in a single organism, in which you sort of have to worry about just that organism-think about it. That organism now can spread its resistance to all these other bacteria that go to lots of different places. So you have, or the bacteria populations have the ability to move a resistance gene, once acquired in one organism, to all these other organisms in all these other niches. So you could have a resistance gene in bacteria that likes to live in your intestinal tract, and suddenly you find the gene in a bacterium that causes pneumonia or meningitis, and it’s the same gene, but somehow, either directly or indirectly, another more dangerous bacteria picked it up.
So when a resistance gene goes from a bacteria in your gut that is helping you to a disease bacteria, it becomes very dangerous, doesn’t it?
Right, an example was in the 1970s when the respiratory tract bacterium Haemophilus influenza was found to be resistant to penicillin for the first time. And when they looked at the mechanism, it was destroying penicillin, and that was not new. What was unique was it was the same gene that had been found in an intestinal bacterium years before. It wasn’t doing much harm there, it was in bacteria that are in our intestinal tract, but we knew it was there. But now, somehow it had moved into an organism that causes disease. But not a disease in the intestinal tract where we could see that exchange. It was now in something that was causing disease in the respiratory tract, and which is normally found there in the lungs. So where did that gene exchange occur? In the person? Did it occur out in nature? It didn’t stop there. That particular gene was then found in a bacterium that causes a sexually transmitted disease called gonorrhea, and it was found in other bacteria causing other diseases. The widespread nature of antibiotic resistance now is so evident that any resistance that is picked up in any organism, we have to say will not be contained. In fact, by the time it’s detected, it has probably already been spread.
What are some of the mechanisms of resistance-how do bacteria utilize these genes?
There are almost as many mechanisms of resistance as genes for resistance. That is saying a lot. But essentially the simplest way to think about it is they destroy the antibiotic in some way or the other. Or they modify it so it is no longer active. Unfortunately for the environment, those genes are not the most numerous. I say that because we’d like for the antibiotic to be destroyed when it is out in the environment instead of sitting around where it is often found, stable, able to select for more and more resistance. But only a small number of resistance traits actually destroy the drug. Most of them are genes that keep the drug out of the cell. They pump them out. Or they modify the target of the antibiotic in the cell. So it’s the ribosome, it protects the ribosome. Or it changes a target in the ribosome so that the drug itself is unchanged, but it can’t work.
Would you characterize this resistance as a moving target?
Antibiotic resistance is clearly a moving target. The more antibiotics we add, the more resistances we see. But I think it is a controllable target. The control is in how we use the antibiotic.
So enzymatically, mechanistically, what do the resistance genes code for?
In all instances, the genes code for a protein that either keeps the antibiotic out, enzymatically degrades it, or is a mutant protein that isn’t able to bind to the antibiotic and so the antibiotic doesn’t get in to stop the bacterium’s multiplication process.
Tell me what eflux pumps are and what they do?
The first eflux pump discovered was that for tetracyclene in the late 1970’s in my own laboratory. It was an unusual mechanism for an antibiotic resistance at that time, and remained a kind of sole new unusual mechanism that was added to the cadre of all these mechanisms, which were much better understood: modification, inactivation. Today there are more eflux proteins known than any other mechanisms of resistance. They come in two flavors: those that eflux a particular family of antibiotics like tetracyclenes or erythromycins, and those that eflux, or pump out, many different kinds of antibiotics. These are called multi-drug eflux systems. The others are called single-drug eflux systems.
The way that you demonstrate eflux is you find out whether or not the antibiotic gets into the cell. Now, you can do that by tagging the antibiotic and looking to see if it ever accumulates in the cell. Or you can take the cell and put it with the antibiotic, then take it out and extract the antibiotic and see if it’s inside. In most if not all instances, this eflux takes energy. So you can also show that keeping the antibiotic out requires energy, and if you don’t give the cell sugar or something to build its energy with, you don’t see this ‘keeping out’ effect. So it’s really an active or energy-requiring eflux, which is the basic mechanism.
Did you discover this by accident, or did you hypothesize this mechanism?
In our studies, we found that tetracyclene was not being degraded. We also thought that it was being kept out of the cell because we didn’t find as much inside as we thought there would be. But it was peculiar, because it seemed like a lot less was getting in than we thought should have if it was just being kept out by a door that was a little bit closed. It could sneak in through other areas. And we then looked at what happened when we deprived the cell of energy, and we found that, sure enough, the antibiotic could kill it. So when we added energy, the antibiotic that was inside the cell was suddenly found outside the cell. So we knew there was something that required energy that kicked the antibiotic out. In fact, it was a membrane eflux system, which as the antibiotic comes in it’s almost like a swinging door; it just never completely gets in. It just comes in and gets sent right back out.
Is this a very site-specific process, or a more general mechanism?
Some drugs can get out of the cell any place in the membrane, and tetracyclene is one. But some drugs require a protein that sort of directs them out, and some of the multi-drug exflux proteins are the eflux pump itself, attached to a little channel that takes you right through to the outside world. And the pump just shoves it right through there. It’s fantastic. These kinds of pumps exist in all different kinds, in all sorts of bacteria. I can say there is not a single bacterium out there for which an eflux pump has not been discovered.
Tell me about your current research here that centers on how to counteract this eflux?
Since the discovery of the tetracyclene eflux system, we had the idea that if we could block it, then we could restore tetracyclene activity. And we showed that with some simple molecules that we made. From this very simple idea emerged a company called ParaTecH Therapeutics, Inc., that I co-founded in 1996, and the company is now actively making new tetracyclenes that either block these pumps or gets the drug around them. It’s a way of restoring the activity of a fabulous class of antibiotics, the tetracyclenes. I think Paratech will do it.
It has become easier to get to this stage with small companies than with the big ones, because Pharma has put a lot more effort in the big profit makers — the areas where people are taking drugs chronically. The acute medicine like an antibiotic doesn’t quite make the profit. So the smaller bio-pharmaceutical companies like Paratech can afford to do this, and a reasonable profit for them is wonderful. And they will provide the public with what we need, our new antibiotics.
Are we at a point now where our science is catching up with what we need to do to counteract these smart bacteria and what they are doing to us?
There are a number of approaches by which we can re-control or regain control over bacterial infections that have become resistant. I say control because I don’t think we should be battling a war against microbes, because they will win. The approaches are basically to find a new, very new, kind of antibiotic that works in a very different way from any of the others, because the bacteria that will eventually become resistant have not yet appeared, because the antibiotic hasn’t been shown to them. If we use such a drug wisely and prudently, we probably can keep it active for a long period of time.
Another way is to take the old class of antibiotics such as tetracyclenes and remodel them into something that is not subject to the resistance that is out there. If we use them prudently we can keep them alive, and it doesn’t matter that bacteria have resistance to the old tetracyclenes, it won’t work on the new ones. So that’s remodeling the old class of drugs, which is a nice thing because the old ones have already proven to be very safe, and they can be taken orally, and they work. So now all you need to do — it’s not all that easy — but you have to make them so they are not subject to the resistance mechanism, which is happening in the tetracyclene field through Peratech pharmaceuticals but is also happening in other areas in terms of penicillins and macrolides. We’re looking for ways to get around resistance. At the same time, these other companies are finding new targets for killing bacteria, and then finding drugs that will inactivate those targets.
What are we as a society-both as physicians and patients-doing wrong with these antibiotics?
It’s very clear that we are overusing antibiotics. We are overusing them in areas where they shouldn’t be used, such as for viral diseases where they have no effect. Colds and flu. We are overusing them for diarrheal diseases, were in fact just waiting and taking symptomatic medication would be enough.
We’re overusing them in animals, in agriculture. We’re overusing them when we don’t need them. And this overuse creates that tremendous pressure on the microbes out there to maintain their resistance. They can’t lose it. They might like to, but why would they? Because with it they live, without it they die. So we are the ones that are kind of directing what they are going to look like. If in fact we can reduce the misuse of antibiotics, and use them only when we need them and we should use them, a tremendous pressure load will be removed.
And for those of us who like to think in the sense of the environment and ecology, it would allow the susceptible strains of bacteria a chance to regain their foothold. When the antibiotic usage is over in a particular patient, the susceptible bacteria will still be there to come back and replace the resistant ones. So we can re-establish the former, susceptible flora that the person had before fairly rapidly. Or better yet, what was in the United States and the rest of the world before antibiotics ever came into being. Because if you have an infection, wouldn’t it be great if you could go back and use one of the two best old antibiotics and still be cured? I think that we can return, somewhat, to those days. But we certainly don’t want to misuse the new antibiotics that are more costly to make. We should be able to use them wisely and prudently so they do their job. The susceptible strains come back, we’ve controlled the infection. We’ve reversed the infection.
Why are doctors prescribing antibiotics for the flu and for viral infections?
It’s a very good question, and a difficult question to answer about why physicians give antibiotics when shouldn’t, when they know it’s a virus. There are two answers. One is, sometimes it looks like a virus, it smells like a virus, but there is a chance it can be bacterial. So let me give an antibiotic. As facts come forth with data that it is more likely viral then bacterium, I think the physician gets more ammunition to say to the patient, this is clearly a virus. We won’t use an antibiotic. On the other hand, it can always be, “call me in the morning if you don’t feel better.” It’s not a life-threatening situation. Then one can also think about developing diagnostic tests that would be really quick that would say virus or bacterium; that’s in the works. And I think quite clearly the patient demand plays a part. There’s a patient in front of the physician, the physician is very busy, and the patient says, “oh, your kidding doc, you’re not going to give me an antibiotic? You know I need an antibiotic.” And the faster they talk, the longer they talk, the doctor says, “well, OK, I don’t really agree, but just in case,” and the prescription is written.
And what happens when a patient stockpiles their drugs? They will save some for later so they don’t have to go back to the doctor to get more. What are the ramifications of that?
It’s important to realize that an antibiotic is designated for bacterial disease, and hundreds of thousands of patients are tested to arrive at a dose you take daily and for a number of days to take it to get rid of that infection. If you don’t take your antibiotic for the full prescription time, then there is some infection left over. There are two problems. One, you might not have gotten rid of the infection. And then you’ve only killed off the most susceptible bacteria, leaving the least susceptible to come back and give you an infection, or worse yet, pass it on to someone else. Now you can’t treat it with that antibiotic. Or two, you have these antibiotics that are left over, which are less than a treatment, but are you going to throw them away? Yeah, I think you should, but most people don’t. They go in the medicine cabinet for the next bout of illness. It may not be you, it may be a child. I mean it’s incredible that people will take it upon themselves to play doctor, but they won’t play mechanic for their car. So why don’t they think about it? You know, antibiotics have this wonderful trait of being safe. It is true. So you figure, “so, I will give it to my husband or my wife, or the neighbor, and there is no harm done because these are antibiotics. They are miracle drugs. They don’t cause problems.” Well it’s not totally true. One person can have an allergy, another one doesn’t. The antibiotic being given is not sufficient to treat the illness, so you could create a resistance problem. And on and on.
So we are diluting the effectiveness of the antibiotic?
We, those who stockpile antibiotics and use the stockpile without a doctor or healthcare provider’s assistance or guidance, is going to overuse and misuse the antibiotic for sure. And it won’t help them, but it will create a resistance problem which is going to be in their home, to be transferred to their family, and then eventually, as more and more families do it, to society.
So your bacteria is really not your own. It can go out into the environment through any number of different ways and start affecting whole communities?
Everyone’s bacteria is shared by everyone else in that environment. We know that when we find in daycare centers the same bacteria in the throats of the kids that are playing together. In households, it’s been shown that the same bacteria are around among household members. So the same thing goes for antibiotic-resistant bacteria. In fact, the individual use of an antibiotic will create antibiotic-resistant bacteria on the skin and intestinal tract while it’s taking care of the infection. After that treatment, we would like for susceptible bacteria to come back, which they should, unless antibiotics are being used so much in that environment. But what has now been shown is that if you’re taking an antibiotic, like say for acne, for 7 to 10 days or more, your usage of that antibiotic affects the other people in the house. This came from Dr. William Conluff’s laboratory of dermatology in London, in which he showed that the skin bacteria of people living in the same household of someone taking an antibiotic for more than a week, for acne, affected not only the kinds of bacteria in the taker, but also in the household members.
This is what I call the ecologic effect, but more so the societal effect, because then each of these people goes out and meets other people, and you are shedding your bacteria. They are becoming part of society. So you are representative of what you have met each day in society, and of what you eat. So your bacteria can change. They aren’t yours to keep. You not only share them, but you can pick up someone else’s. And so I think it’s surprising to people to find out that, even though they have never taken antibiotics or have taken very few, that their intestinal tract is still loaded with bacteria that are resistant to many different antibiotics, as we have shown.
How big of a problem is that to society?
It’s a huge problem to society because it provides a reservoir of these resistance genes that can be exchanged like baseball cards with each other, all the bacteria. Because you give me yours, I’ll give you mine. Then bacteria become multi-drug resistant, and we’re harboring them, and then later, when we get an infection, there is a better likelihood, a high likelihood now, that it will be resistant.
If a strain of resistant bacteria shows up in a community, let’s say it shows up in a school. What should the public health people be doing to control it?
If I were looking at an antibiotic resistance problem, the first thing I would look at is how antibiotics are being used. I would find out if the usage is correct. I would find out if the levels are correct. Because low-level usage is the best way to create resistance, because bacteria aren’t quite killed. So they can mutate easily or acquire resistance genes. So that would be the first thing I would look at. The second thing I would look at is, how much contact do the people have with each other? And can we institute more washing of hands? And more washing of instruments that are being used. I am not talking about impregnating them with antibacterials, but just washing with soap and water. That is all you need. So you do a little infection control. I would say you would reduce the resistance carriage.
Wouldn’t you have to first identify the strain of bacteria?
You certainly want to know the bacterium, because then you know where it lies and likes to be. I mean is it in the throat? Is it on the skin? Is it in the intestinal tract? Because without that information, you wouldn’t quite know even know what antibiotics to look at and where to look to see if you’ve been successful, and what you should institute to avoid the transfer.
And I guess public health officials, and all of us, should be practicing better surveillance all the way around.
We, the Alliance for Prudent Use of Antibiotics, is very actively, aggressively pushing surveillance as a local measure. It may be interesting to find out that in India or Pakistan or Russia there is a problem with multi-drug resistance x, y, or z. But how does that affect my community here in Boston? And it may be in Boston but not in Brooklyn. But you really need to know what the local resistance patterns are, and that can be done. Resistance is a local phenomenon, but it’s global in its presentation. You might have a different problem resistance in one town to the next. We all have resistance. But it stems from different antibiotics being used, the societal makeup, how many daycare centers we have, how many nursing homes we have, all of that combined.
Essentially, in order to get a resistance problem for a community, you have to be close together. We did studies in Nepal where we showed that you didn’t have to take the antibiotic to have resistance. You just had to be near or in a city where a lot of antibiotics were being used. That’s sort of what we see here. In the communities outside of Kathmandu in Nepal, they might have been taking antibiotics, but their resistance levels were very low. That’s because there was a lot of separation. They were individualized. They weren’t in a dense situation, where there were lots of medical centers and lots of antibiotics being given. So that they entered in and out of those environments, which were filled with resistant bacteria. So you and your carriage of bacteria represent what is in the environment in which you interact. If you’re living on a farm, I would guess you would have a much cleaner resistance profile, unless you are using antibiotics for the animal industry.
So once it shows up in a community, how fast does it spread? It sounds like it just depends on what the community is made up of?
There are studies to try to understand how fast or by what routes bacteria spread in different environments. In the hospital, many more studies are made, because it is closed. In a school too. In an environment as broad as a society with homes and houses, do they occur more in cities where they are living closer in apartment buildings? We aren’t doing those studies. We can only imagine that it is quicker. We look at tuberculosis and we see that it spread much more easily in confined areas where all these people were put together in housing in New York. Not in the wide-open areas of the country. So it is human-human contact, the time period that occurs over, and how much it occurs. And what’s the geographic density that will express itself in resistance spread.
I want to touch on agriculture and animal use. Why are we feeding animals antibiotics? What are the ramifications of that?
Sometime in the 1950s, the agricultural industry found that feeding animals the leftover carcasses of bacteria that make tetracyclene helped them to grow better. The investigators were convinced that this was an unusual nutritional factor. And it was intially touted as a new growth factor until other investigators showed that it was trace amounts of the tetracyclene that had not been fully extracted from these carcasses. Well then, why bother only with the carcasses, let’s just add back a little bit of antibiotic, because we think it’s working as a vitamin, not as an anti-infective, because it’s below the therapeutic amount.
That started a whole industry, from the 1950s, of sub-therapeutic, less than therapeutic amounts of antibiotics, mainly pennicillins and tetracyclenes, being added back to animal feed to help the animals grow faster, on the same amount of protein or feed. What was missed at the time was the fact that even this amount of antibiotic is enough to select out resistant forms of bacteria. So under the guise of being helpful to the industry, what was happening was that bacteria associated with the animals and the people living on the farms were becoming resistant to the antibiotics, and in many instances to other antibiotics, even though they were not in therapeutic amounts. Because in fact, even being sub-therapeutic, they still were able to treat a lot of bacteria and stop them from growing. Those that were resistant emerged, and they became plentiful.
So then, in the 1970s, when investigators looked at the levels of antibiotic resistance in farms that used antibiotics versus those that didn’t, they found a huge difference. Resistance was so commonplace. Not only in the animals and the animal feces and the environment of the animals, but in the people working on the farm. So we knew then that the antibiotics had a local effect on that farm. It then moved to the fact that the antibiotic-resistant bacteria, if they caused diseases like salmonella or camplobacter, could be traced in the food that someone ate in a house far away. They found it was resistant, and they could go back and say, well, it came from this farm where they are using antibiotics.
You mean they ate meat from that farm?
Of course. Chopped up, the meat goes to slaughter, whether it’s beef, pork, poultry, turkeys, you name it. And bacteria are always associated. You can’t keep bacteria out. So although you clean the carcasses, there is intestinal and skin bacteria that can still come along, and what you end up with is a meat product that has bacteria around it. And if you cook it, you get rid of them. But if you put them on a counter, and then you sort of wash the counter a little bit and start making your salads on the same counter, you just keep the antibiotic-resistant bacteria flowing into a new form. Then you eat the salad, and you got ’em.
Or if you make hamburger, as has been often been the case, the hamburger meat takes the outside of the meat, which is loaded with bacteria, and grinds it up to the inside. Then if you don’t cook the hamburger in the center to a certain temperature, the bacteria survive. That’s of course how a lot of these toxic bacteria have been spread, in hamburgers, because they are not fully cooked.
So this is a sort of balancing act, because there are the good bacteria and the flora you have to maintain too. I know you don’t like to call it a war on microbes, because we need them to survive. How do we reduce these reservoirs of resistance genes? What’s our strategy here?
There are two strategies to kind of reverse this huge reservoir of resistance genes. One is, of course, to begin to use antibiotics more prudently. In my mind, there is a threshold that you can give a lot, a reasonable amount, of antibiotics and still allow the susceptible bacteria to come back. But once you go above that threshold, the susceptible bacteria are so far away. They don’t have a chance to get back into that environment before you’ve used the antibiotic again. Even when you stop it, the resistant bacteria are still there when you come back for another treatment. It could be 6 months later, it could be 12 months later — it is not enough time.
The other approach, which is alternative, it’s not fully accepted but perhaps will gain ground, is to purposely add new susceptible bacteria to that environment. As an example, yogurt contains a bacteria called Lactobacilis acidophilus; for years people have been told that after you have an antibiotic treatment, take yogurt. It turns out that not all yogurt is the same, and very few yogurts have enough live bacteria to really do the job. But there are certain new forms of Lactobacilis that you get in preparations that are able to return the flora to a natural flora, and these can actually treat diarrheal diseases without an antibiotic, and they actually have been effective in treating other diseases.
There is a mounting interest, too slow for my taste, in biotherapy. Pro-biotics-it is much bigger in Europe than in the United States. But I mention it because I can see using biology rather than chemistry to deal with some of the problems on which we really rely on chemistry. If we can get friendly strains of bacteria that we can spray in the hospital room after we’ve had a Staph aureus or endococcus, and we can’t really kill it fully with the sprays of chemicals-I mean we just can’t. It’s hiding somewhere. But if we were able to spray the room with a bacterium that could get into every nook and cranny, could grow, could get inside the telephone. You know, all those places that chemicals won’t get, and just crowd out the bacterium we don’t want. We could control it without a chemical. Now I realize that this is kind of heretical, but it pushes the button a bit. I would like to see more studies on restoring the natural environment, prospectively, aggressively. Not just by withdrawing the agent that has caused the issue, but actually by adding another one back. We have done studies like that.
Well, that’s like bioremediation, just as we are using bacteria to clean up mines and toxic waste dumps.
Right. We should use biology to treat biology, not just chemistry. So we can use biology to try to control a disease. In malaria, for instance, there has been a proposal to use a breed of mosquitoes that is not able to be infected by the malaria parasite and get them to take over the environment where malaria is rampant.
So we thought we had infectious diseases under control with these miracle drugs, but the antibiotics really have been their own undoing-or not the antibiotics but how we’ve used them.
But it is the antibiotics. The first title I used for my book was The Antibiotic Paradox: How Miracle Drugs are Destroying the Miracle. Because their use has led to their demise. It’s like they’re sowing the seeds of their own destruction, and you have all sorts of little sayings that fit with what is happening. It’s because they are so good. I mean they will kill bacteria unless they can survive them. And if they survive, then they survive with genes that will allow you to counteract their effects. So they destroyed the miracle by selecting out those bacteria that will resist them. But more than that, these resistance genes are transferable to others.
So it’s not just that, so what, we have one bacterium that is resistant, or one little community. It’s only them, but think of all the others. Because once they are there, they can transfer to all the other bacteria. So in fact, over-use of an antibiotic in any area can create resistance in many different types of bacteria that could cause different types of illnesses in different people. And of course, the people that are most vulnerable are those undergoing the most advanced therapies for cancer, those with transplanted organs. We’ve done some fantastic things in medicine and surgery. New hips, new other joints, and what happens is, if they get infected, they’re hard to treat if they are resistant. The resistance problem really hits at the most vulnerable of our population. But those that are undergoing the most modern of our treatments, those for cancer, those for replacement of organs or replacement of limbs, where an infection with a resistant bacteria can totally reverse the pleasures and the rewards of that operation or that therapy.
These bacteria can be bacteria out there that are innocent bystanders. Because people who are compromised get infections by bacteria that wouldn’t hurt the normal person. But they are the ones that have become resistant because of the overuse of antibiotics in other ways.
So bottom line, we obviously need a broader awareness of this whole issue?
For me, the global awareness was evident in the early 1980s when the Alliance for Prudent Use of Antibiotics was created. Unfortunately it has taken a long time to get people to accept the fact that this problem is not going to go away; that we can’t keep up by making newer and newer antibiotics that we might or might not have, and then begin to use them the wrong way as well, so that the bacteria respond with resistance. But people have their own ways of thinking. And it’s very hard to change a lot of the population today. So part of what we’re trying to do is reach the students. I think that as students, high school and younger, learn of the powers of antibiotics they should also learn about the problems that can ensue. They will understand that antibiotics are used for bacterial infections. They are not for colds, they should be precious drugs. Not aspirin-like; they don’t do everything. That in fact, it’s reserving them, respecting them for the purpose for which they were developed that we will be able to reverse the resistance problem. And I hope that new generations of physicians and consumers and nurses will have a better idea of what the miracle drug is and how to use it.
What is the problem with household use of antibacterial disinfectants?
The problem is, we’re increasing awareness of antibiotic misuse and antibiotic resistance, but there is an undercurrent of marketing of products that contain surface antibacterial chemicals to treat these problem microbes. And it’s counteracting our trying to get awareness to the people that bacteria should be around. We shouldn’t try to destroy them. And here we have these products added to normal soaps and disinfectants which have at best no effect, but have at worst an effect on the environment. There are no health claims for these products. Studies that have been done do not show that they have added benefit health-wise, to the healthy household. In cases of patients who are vulnerable to diseases, like cancer patients, AIDS patients, elderly diabetics, they play a role. Then they need to be used for minutes, not the few seconds that the normal person uses these products in the home. So what worries us is that, one, the message gets around that all microbes are bad and we have got to wipe them out, which means antibiotics aren’t so bad either. And the other thing is that we are creating an environment of bacteria that are resistant to these products, and then may well be resistant to antibiotics as well.
If they have, for instance, these multi-drug eflux pumps or mutations in genes that are also targets for antibiotics, they may be resistant. So there is a connection, but there is an unfortunate mounting rage for antibacterial chemicals added to normal cleansings. And I think that this will create a changed microbiology and very likely, at least in the laboratory, contribute to the propogation of resistant bacteria.
What other questions do we need to ask on the horizon?
Probably for me the most important question is, what is the relationship between the amount of antibiotic used in a particular environment and the emergence of resistance problem. I like to think that there is a threshold, a total amount of antibiotic that you can use in a house, in a hospital, in a society. It will be different amounts in different situations. But you want to affect the cure but you don’t want to change the microbiology permanently. We don’t have those data. What is that amount? Is it different for arithromicin, versus tetracyclene, versus pennicillin? And those are the kinds of studies that would help us, because then a hospital could monitor, how much of this antibiotic is being used in this environment? Even on this floor? And they could say, “wait a minute, we’re getting close to a level where resistance could emerge.” Or in the house, or in the patient. I find it a mistake when there is a recommendation to use the same antibiotic for every illness. Often that comes through in environments where antibiotics are not readily available, because of cost and they say well use this one. Well that’s a mistake. Because that then will pervade-that single antibiotic usage clearly will select for resistant bacteria.