



Rediscovering Biology: Molecular to Global Perspectives
HIV and AIDS Expert Interview Transcript: Laurie Garret
 Journalist, Newsday
Journalist, Newsday
Garret is the author of the books The Coming Plague: Newly Emerging Diseases in a World Out of Balance and Betrayal of Trust: The Collapse of Global Public Health. She is also a medical and science writer for Newsday, in New York City. For her work, she has been awarded The Peabody, The Polk, and The Pulitzer Prize.
Interview Transcript
Garret is the author of the books The Coming Plague: Newly Emerging Diseases in a World Out of Balance and Betrayal of Trust: The Collapse of Global Public Health. She is also a medical and science writer for Newsday, in New York City. For her work, she has been awarded The Peabody, The Polk, and The Pulitzer Prize.
How are new diseases emerging and old diseases re-emerging?
Well first of all, diseases are not newly emerging. This has been going on for a long time. It’s just that we were in such a state of arrogance as a species, we humans-especially we humans in the wealthy world coming out of World War II. We really believed we were vanquishing or had vanquished most of the microbial diseases. And we spoke of total elimination of all infectious diseases as late at the early 1970’s here in the United States. And all the while of course, diseases were newly emerging and continuing to emerge in the poor world. It’s just that we didn’t care about the poor world. When we talked about the elimination of infectious diseases, we were really only talking about the wealthy world, and were ignoring by far the majority of the global human population.
Now we’ve reached a point where people are a lot less sanguine about eliminating all infectious diseases, and we’ve come to understand, finally, that microbes evolve far more rapidly than do humans. That they are constantly adapting to whatever circumstances we throw their way. They are constantly developing resistance to the antimicrobials we use to target them. And furthermore, we are their best allies. We are aiding and abetting the microbes constantly by providing them with new opportunities to come into our population in various ways. The thing that has really escalated matters considerably is globalization.
What globalization is about, from the point of view of the microbes, is that we as a species, we human beings, are now on the move constantly. We are urbanizing at the most rapid pace in the history of our species. So by the middle of the 21st century, the majority of the Homo sapiens population will be living in cities. Less than 10 years ago it was a clear majority, roughly 70% that were living in rural areas. So this urbanization is occurring at a rapid pace. Mega-cities are defined as a city with 10 million or more people in them, and the United Nations population fund says there will be 23 of them in the world by the middle of the 21st century; of those, only four will be in developed countries. So the remainder will all be in poor countries that lack the resources and the financial capacity to build safe infrastructures in these cities. I have traveled in all of them. I know what they look like. We’re talking about microbe heavens. We’re talking about ideal circumstances for the transmission of disease. There is a lack of sewer systems, a lack of safe water, a lack of paved roads, a lack of drainage systems, so you get pooled water for vectors-for mosquitoes-and so on. There’s a lack of hospital facilities. And there is horrible, sub-standard housing for most of the population, which is newly arrived in these cities, living in lean-to shacks and jerry-rigged shelters of one kind or another. All of this leads to extraordinary opportunities for the microbes.
If you add to that, that we’ve globalized the production and distribution of food so that more and more of what Americans are eating, particularly during our winter, is grown in some developing country somewhere. And that introduces microbes that come from that country’s ecology, newly introduced into ours. We are globalizing meat production, so that we’ve seen the foot and mouth disease and the prions with the mad cow disease from Europe. That is becoming a problem more and more all around the world. The United States has exported in food products E. coli 0157, which causes hemolytic urea and is roughly the most difficult form of enteric, or stomach, microbial disease that we’ve introduced into the world in quite a number of decades.
What you see then is that we are creating a perfect opportunity as we go into the depths of the 21st century for microbes to find their way into ecologies that they’ve never been in before. The most dramatic example would be the West Nile virus. Here is a virus that has a normal ecology that requires a sort of swampy interface with savannah in northern Africa. It is carried by African mosquitoes. It’s not found much of anywhere else in the world. Who could have imagined that this would have emerged in 1999 in the concrete jungle of New York City? It was carried by indigenous North American mosquitoes and ended up being, three years down the road, in the majority of American states, having found its way in a whole diverse range of ecologies all across North America. Now fortunately this is not a terribly lethal virus. And fortunately, most people are readily able to develop immunity if they are bitten by these mosquitoes that are carrying it. But what that is telling us is if this could do it, well, let us recall that in the history of North America two of the biggest killers were yellow fever and malaria, and we still have all those mosquitoes.
Why is malaria continuing to kill 3 million people a year? Why is this disease not eradicated by now?
Coming out of World War II we had all the tools necessary to eradicate malaria. We had a brand new, totally effective pesticide called DDT that killed mosquitoes 100% of the time. We had a fabulous new drug called chloroquine that both could prevent one from developing malaria in the first place or getting infected, and secondly it could treat the disease if you had it. Both DDT and chloroquine worked all the time. We set out as an international effort to eradicate malaria from Earth using these two powerful tools. Congress stopped the funding after three years. We were close, in many parts of the world. We certainly did manage to eradicate it from North America and most of South America. In fact, except for a couple of pockets deep in the Amazon, malaria was gone from South America. We had virtually eradicated it from major parts of Asia, and of course from all of Europe. Most Americans today don’t realize that malaria was a major killer every summer in Italy, Greece, and Portugal-all the way up to St. Petersburg, Russia. We had pushed it back.
Then we realized again, the microbes had capacities that we always underestimate. The microbes, the parasites themselves, began to develop resistance to chloroquine, and the mosquitoes developed resistance to DDT. And both tools became less and less effective. Then of course the ecological impacts of DDT came to be known, and there was a widespread belief that we should no longer use that compound. Nothing has come along that is better than DDT, in terms of using it in the environment to decimate mosquitoes. So we haven’t got a ready replacement for DDT, and we have gone through several additional lines of medications trying to find something that can fill the void left by the resistance against chloroquine.
And what we’ve seen is resistance has appeared against every additional drug as we have brought it into play. So now in Southeast Asia in particular, we have multi-drug resistant forms of the malaria parasite that actually can defeat pretty much everything we throw their way.
So what are we supposed to do about this? We can’t really prevent emerging diseases from happening. How can we control these emerging diseases?
Well the good news is that most spread and emergence of microbial disease is our fault. We are providing the opportunities for the microbes, which means it’s correctable-if only we had the political will, the economic will, and a little less arrogance as a species. We have to realize that we live in a microbial soup. We’re surrounded by microbes. They are all inside of us. We haven’t even come close to identifying what they are. I was recently at a scientific meeting, where it is estimated that we know less than 1% of the identities of all microbes in the world. So it is arrogant in the extreme to imagine that we can bring them under our control. A much smarter way to approach living in this microbial soup is to ask how you can do so in a reasonably defensive manner. For example, many of your viewers will probably say, ah, that’s why I need anti-microbial soap, and I need to scrub my kitchen with the strongest possible disinfectant every day and so on, so forth. Au contraire: you’re going to breed resistant strains of microbes. We have pathogenic bacteria that can grow on a bar of soap because they have become so resistant. No, what it means is that, yes, you keep a clean home, but you’re rational about it. You don’t use a wooden cutting board in your kitchen to cut meat knowing full well that if there are microbes in the meat they can go into the wood and then go on the fresh fruit that you subsequently cut on the same board.
You know, it’s just common sense. It’s a matter of understanding the microbes: how they spread, how they cause disease, and to take precautions against that. The classic example is the period in Japan in the last decade when many Japanese became very microbe-phobic, and started wearing masks around in the streets, which was very silly. In fact, very few of the microbes that are really threats to human beings are passed so readily in the air that just simply by being in the same breathing space as someone could result infection.
But what they weren’t thinking about is, in the winter, why do you think we have flu and colds so much in the winter? It’s because one person who has one is rubbing their nose and touching a doorknob. To protect yourself, wear gloves when you’re in public places, or wash your hands more frequently to protect other people when you’re sick. These are basic, obvious things.
What about in terms of a bigger picture-particularly in dealing with West Nile virus and malaria-how important is it to have a good public health strategy in place?
I’ve spent a lot of years looking at the state of the public health infrastructure both domestically and internationally. When I wrote Betrayal of Trust, my sense was that we were in a really catastrophically vulnerable situation. Interestingly, our Congress recognized that, but not until a vital envelope was opened in Senator Tom Daschle’s office that contained anthrax. It was that moment when Congress said, “Oh my gosh, who is supposed to protect us?” And by golly we’ve been cutting our public health infrastructure budgets for decades, and suddenly they woke up and found out that 45% of our public health offices in the United States didn’t even have a FAX machine, that there was no standardized laboratory equipment or test methods for finding potential epidemics in any of the public health laboratories across America. Every public health laboratory, not just in the United States but pretty much in the whole world that I have been able to talk to, have said those simple, five envelopes with anthrax resulted in every laboratory in the world being overwhelmed beyond capacity to respond to envelopes that looked suspicious, and everything from leisure chairs to brief cases were coming into labs from people saying, “there is a white powder on it. What is it?” Suddenly we’ve had a bit of an awakening.
Following the anthrax assaults, President George W. Bush created a whole budget initiative to try and vastly improve the public health infrastructure in America. We’ve put nearly a billion dollars into it now, as of the summer of 2002. And there may be more going in. I think now what everybody realizes is that the weak spot is a two-fold problem. One, we’ve so under-valued public health and public health skills in this country that our public health personnel are grossly under-paid. They are so grossly under-paid that they have poor morale, little incentive to over-work and put in those midnight hours during an epidemic unless it’s very personally, altruistically motivated.
Meanwhile, in our hospital system, that crucial interface between the clinical world and the public health world, we see pay scales plummeting. We have a vast desperate shortage of nurses. We now know, and it’s clearly documented, that wherever we have a shortage of nurses we have a higher incidence of hospital-borne disease. That means you check in with one problem, a heart attack let’s say. You check out with another, an infection you acquired while you were on that hospital ward, awaiting a bypass operation. That may in fact kill you or result in permanent injury of some sort. So we have a terrible problem that throwing a billion dollars out to buy more FAX machines and build better labs won’t solve. It’s a personnel issue.
The other weak link that we now understand, and that even conservatives in Congress are beginning to appreciate, is the international connection. When you get down on the ground in poor countries, as I have for years, you will see that the infrastructure is a laughing stock. What we see at the local level is entire laboratories trying to operate with 6 or 7 test tubes, a bottle of alcohol and a couple of pipettes. Here we are talking in the United States about trying to put in public health laboratories automated DNA sequencers. In most of the developing world, it really boils down to, “do you have one guy who knows how to use a few test tubes, a couple of pipettes and a Bunsen burner?”
So what are the global ramifications if we don’t start paying attention to the problems in developing countries?
It’s consistently been a problem to understand as Americans why we have some kind of duty, or why it’s in our own interest, to care about people in Bangladesh or Angola or a country we can’t even pronounce, and most of us don’t even know where to find it on a map. It’s been an ongoing issue to try and understand how much of this is a national security concern? How much of this is just about this sort of Judeo-Christian spirit and caring about humanity? And how much may be at a very basic level about the safety of your own family? And right now there is quite a struggle going on over those three points, in terms of reaching out, not just to the United States but also to the EU and to Japan, to all the wealthiest nations of the world to say, “we’ve seen a tremendous skewing in the distribution of wealth in this world since the fall of communism. The wealthy countries have become much, much wealthier. The United States, Northern Europe, and Japan control more than 50% of all global wealth right now. The United States is approaching 35% of all global wealth controlled by one country. We, the wealthy world, represent less than 5% of the global population. Yet the needs are clearly in those desperately poor countries that can’t possibly repair their public health catastrophe without outside assistance. So how do we get money from where it now is to where the needs are? In a way, that doesn’t sound like a call for global socialism or something else equally absurd. It’s a real dilemma.
There are more and more people in our Central Intelligence Agency, our National Security Council, and other equivalent private and public institutions that deal with national security that are looking in particular at the HIV pandemic. But they’re also looking at tuberculosis, malaria and other areas, and they are saying, “These are national security issues. Our future capacity as a global power is threatened by these diseases.” Secretary Powell in particular, the Secretary of the State, has made this a major issue and has raised it repeatedly. Kofi Annan, the Secretary Director General of the United Nations has made this a hallmark of his 3rd tenure running the UN. But that argument will only go so far. I think bottom line is that we also have to talk about global citizenry.
Americans are incredibly generous people. When we see film footage on CNN on a famine in Ethiopia, and you look at the dollars that pour in from individual checking accounts, not from governments but from individuals who sit down, people see it, they cry and they write a check. Americans far, far out-donate compared to Europeans or anybody else on Earth. The truth of the matter is that if there is a crisis in the world and you need the individual to go to their checking accounts, every international humanitarian relief organization knows the ball game is the United States of America. But, that is not enough money. The scale of what we are talking about is not something that everybody watching this can go off and help solve with one quick check written with a sense of urgency one afternoon. We are really speaking about a much more ongoing, sustained, decades-long effort that is the kind of thing that has to be put together by a combination of powerful private interests and governments.
What happens if we don’t start paying attention to research and vector control and surveillance immediately?
The best way to understand what is at stake here and how it will affect us as Americans is to look at HIV. It’s interesting to me, having begun covering HIV before it had a name and before we even knew it was infectious in 1981, and having lived in Africa shortly before then, not knowing AIDS was already there but having seen the behaviors that have resulted in the rapid spread of this disease. It’s interesting to me to see that we have to get 22 years into this epidemic before government institutions at the highest level begin to appreciate the catastrophe for what it is. That means that we have given these microbes a 22-year head start. We are only just beginning, just at the first baby steps of beginning to understand what it is going to take to bring this epidemic under control. We may not even have time. We may have waited too long. But when we look at the kinds of scenarios that are now being promulgated by national security experts, historians, political analysts an so on. We can already see that AIDS is going to be the number one destabilizing factor for Africa, for years and years to come. It already has dramatically hurt the economies of the hardest hit countries. We’ve seen the gross domestic products of these countries go backwards radically. We have seen life expectancy plummeting in many of the countries of sub-Saharan Africa. Life expectancy today is at World War II levels and moving backwards towards the 19th century. Not forwards into the 21st. GDP growth, same thing, it’s heading backwards. All development indicators are heading backwards. Literacy is plummeting. Child health is falling, not just due to HIV, but secondarily you see more and more AIDS orphans going unvaccinated. So you are seeing resurgences in measles, in polio. All these diseases that in our arrogance we thought we would completely have eradicated by now. Now we have poof that they are coming back.
Why don’t the developing countries understand what causes AIDS and change their sexual behavior? And two, do you think Americans are getting lackadaisical in taking if off our radar screen?
Well, you know, many people ask questions about sub-Saharan Africa and why HIV has managed to take hold to the degree that it has. The first thing I would point out is that right now the most rapidly growing epidemic of HIV on Earth is not in sub-Saharan Africa, it is in the former Soviet countries-in particular, in Russia, the Ukraine and the Baltic states. I’ve spent a lot of time looking at that epidemic. That is almost a 100% IV drug use-, narcotics-driven epidemic. Hey, that’s a no-brainer. That is an easy one to stop. Make sure that everybody uses clean needles and start building up methadone programs and drug rehab programs to get the kids off the narcotics in the first place. Guess what? They won’t do it. They won’t do it because of the same reasons we in America have a hard time dealing with drug abusers. There is a greater hatred of the drug users than there is of the virus. They’re willing to risk having the societies overwhelmed by AIDS, rather than do anything to reach out and assist a drug user. Hey, why should Russians think any better of a drug user than Americans do? Most Americans would happily see drug users drop dead. So again, the microbes are able to exploit our own prejudices to take hold in a society.
Current projections from the Russian ministry of Health are that by 2010, a very short time away, roughly 10 to 12% of all Russians will be HIV positive. The Ukraine is looking at roughly the same thing, as is Belarus. Up in the Baltic’s, we see roughly the same projections. So we are talking about an African-scale epidemic about to take hold in a region that is enormous-with 11 time zones and highly complex societies with tremendous public health resource scarcities-these are really damaged infrastructures in the post Communist world.
If you look at Africa, where heterosexual transmission is overwhelmingly the reason for the epidemic, this is a far more complicated and difficult problem. I mean, it’s one thing to say to a drug user, “I may not like that you’re addicted to narcotics, and I may not like that sometimes you steal and so on to buy your drugs, but here is a sterile syringe-at least don’t pass on your virus to any other drug user.” It is another to try and say to an entire society, “Change all the sexual mores that have been the norm for hundreds of years, and become a new kind of society with an entirely different sense of gender balance, of empowerment of women, of a right of refusal of sexual intercourse, of the value of the female gender, and overnight transform yourselves into an entirely different culture.” It’s not going to happen.
I think the real problem here is that it has taken this long, that this epidemic started in the early 1970’s in Africa. It’s taken this long to get to the point where the issue of gender is even on the agenda. But number one driving force for this epidemic in Sub Saharan Africa and increasingly in Asia is the extraordinarily low power balance on the side of females. Most women have no right of refusal of sexual intercourse. They have no ability to dictate when, where or with whom they have sex. Rape is so commonplace that it is only recently being thought of as a criminal activity. And men quite commonly have well over 10 women as regular partners in their lives, with one being the wife that officially bears their offspring. In that kind of a setting this virus, again, has found that human beings have offered it the perfect opportunity for rapid spread. And it’s going to be very, very difficult to turn that around.
Well one society, Uganda has begun to turn a lot of this around. It is interesting that people have made a lot of the fact that President Yoweri Museveni himself has for many years been speaking about HIV. And he has been the most aggressive head of state in the whole world in terms of addressing HIV and alerting his own population, and trying to defeat denial constantly. But there is another factor that has played a big role in Uganda. That has been the rise of a sense of anger among the women, a demand for accountability from their husbands, from the men they have sexual relations with. They’re trying to teach their sons to behave differently.
We’ve seen, for example, there is just new data out showing that as little as 5 years ago about 8 % of Ugandan men were polygamists. Now that is a big drop from when HIV first came in. More interestingly is that just in the last 5 years it has dropped to about 2%. That means that a lot of women have managed to get a little more say so, and a lot of the men who were polygamists died, and that served as a glaring example to other men that as much as you may like having 18 women, regulars in your lives, here is the risk. The grave. Not just the grave for you but for your children, for all those wives, all those girlfriends, and pretty soon there is nobody left in the village. But Uganda, which by the way has the oldest part of the epidemic, yes, they are ahead of the game, but they have been living with this a lot longer than most of the rest of the world. It’s taken three human generations, and in fact the beginnings of the fourth, for Uganda to get to a point where the kind of social upheaval that’s necessary is beginning to happen.
And we can’t imagine that that is what is going to have to happen everywhere else in the world in order for change to occur. Let me give you a flip side. Let’s take a look at Botswana. Botswana, prior to its current HIV disaster, was the best-case scenario from the point of view of the World Bank for economic triumph in sub-Saharan Africa. It had a rising GDP per capita. The economy was booming. It had a democracy. The World Bank, CIA, everybody, NATO, they all thought Botswana is our little darling. They have a tiny population-about one and a half million people. Much of it is at high altitude, so there is a low malaria background problem. There is a diamond industry. It was looking great. Everybody was very excited about Botswana. Today in Botswana, the adult prevalence of HIV is 44%. Think about what that number would mean. If 44% of the students in your high school were HIV positive, imagine the morale. Imagine what kind of future are you even talking about in the classroom? Why should they even bother to be in the classroom? What’s in it for them? Hey, odds are 50/ 50 they are going to be dead before they ever have to do an algebra problem.
So, here is this country once thought to be the real success story of sub-Saharan Africa, and they are looking at roughly 50/ 50 odds that any individual who is between 15 and 40 years of age is infected. What we have already seen happen can give us clues about what can happen to the whole continent. Eventually it could happen to India, to China, to Russia, to Ukraine, to all these hard-hit areas of the world. Well, first of all, astonishingly, surveys of pregnant woman not only show of course that roughly 44% of them are infected, but it also showed a little known and observed fact: that 80% of them are giving birth out of wedlock. Now that tells you social collapse has already happened. The whole institution of marriage has disappeared. Couple that with the fact that among the people that everybody is losing are the heads of the police departments, the top elements of the military, the best trained government officials, most of your lawyers, what remained of your doctors, your schoolteachers. Schoolteacher incidence actually tends to be among the highest all over Africa. And of course you lose your parents. So then you get what demographers call a chimney effect.
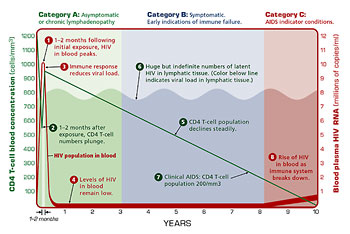
Here’s what happens. Let us imagine that I have an access here, as I go up, I am looking at age. Well at the top you still have between age 60 and 80, roughly the same size population as you would have in the absence of AIDS. It’s a little tiny chimney sticking up. Then you notice that the chimney keeps going down to about 35 years of age. So missing is what ought to be this big bulge that is your middle-aged population. Instead, it keeps going down, sliver, sliver, sliver, meaning there is no labor force, no parents, no mentors for kids, and then suddenly there is a bulge at about age 30 that goes way out to about age 13. This big bulging population of unsupervised, unguided, untrained, unskilled, teenagers and young adults. And as any schoolteacher knows, what does an unsupervised teenager do? Well let’s just say he does everything that facilitates the spread of HIV.
Can you talk for a moment about the scope of the problem and some of the initiatives to help abate it, such as vaccines and other initiatives?
I think we have to step back for a moment and think like historians. You know, if you teach history to students, the one thing you really want them to end up coming away with is a tool set that allows them to look at the present world with the lessons of the past in mind, with some ability to imagine a future. So that any given problem they might want to address in their lives, they can see with this kind of historical guidance.
So if we take that perspective and apply it to HIV, the first thing we immediately see is that this epidemic has dwarfed everything that ever afflicted humanity before now. It has now well eclipsed the 14th century black death, the 1918 influenza pandemic and anything else that we know of that has ever hit humanity, that this is number one.
Number two, if we look at what impact both the flu and more importantly the plague had on humanity, we see that huge mounts of social institutions were fundamentally changed. The plague ushered in the Renaissance. It ushered in a complete collapse of Catholicism’s control of Europe and ultimately of the aristocracy. It ushered in the reformation and a kind of sense of skepticism and doubt among the masses in the absolute control and capacity of this ruling elite that controlled them. Because the ruling elite couldn’t defend them against the plague. The ruling elite offered no correct answers to slow that pandemic down. Barbara Tuchman describes this in her work of historical fiction, A Distant Mirror, a book I highly recommend. And what we can see now is that HIV is undermining all sorts of institutions in the same profound way.
I think first of all that we have no specific historical lesson to draw on; this is unprecedented. This is on a scale that just almost is beyond the human capacity to imagine. This is a science fiction level. Secondly, we can see that because this is a virus that specifically attacks the immune system, the secondary and tertiary effects of this just in a disease perspective are unimaginable as well. It already has created a massive global tuberculosis pandemic as its companion. We don’t know what might be next. It’s already pushing Hepatitis C. It may very well be that there are other microbes that are ready to pounce and take advantage as a large-scale immune dysfunction occurs in other ecological sectors of the planet. For example, HIV is now beginning to take hold in Indonesia. Well, Indonesia is home to a lot of microbial diseases that really are bizarre and poorly understood and that may be able to surge once there is a critical mass of immuno-deficient people in a population.
Just think, for example, of what we’re going through right now in bio-terrorism preparedness in this country, where we imagine there might be someone unleashing small pox someday. And all of a sudden our public health infrastructure is realizing that immunizing the American people in 2004 for small pox is not like doing it in 1964, because in 1964 we didn’t have a huge immuno-deficient population in America. We didn’t have people with HIV. We didn’t have cancer patients being kept alive on a massive scale with chemotherapy and radiation that had debilitated their immune systems. We didn’t have a huge senior citizen population living well into their 90’s with highly deficient immune systems. So all of the sudden, we’re trying to imagine, “How do we do mass vaccinations? Can we even do it to the level that is required to achieve herd immunity?” You know it’s much more complicated in 2004 than it would have been in 1964, or ’54 or ’44. And if you begin to spin this out and imagine this on a larger and larger scale, you can see the many, many ramifications occurring in America.
Here’s another kicker to consider: we treat our HIV patients here and we treat them very well. People are living very long lives carrying this virus. They are also continuing to pass the virus: by no means has the availability of treatment slowed this epidemic. On the contrary, all evidence indicated that they are more people getting infected every day today than was the case 6 years ago.
Is that what you mean when you say one of the problems with HIV is that it has been medicalized-that we treat it as a treatable disease rather than a societal problem?
Right. We haven’t, in North America or Europe, come to consider HIV a chronic disease. The model is, “Oh, it’s like diabetes, you take your insulin and you stay well.” But it’s not like diabetes, because diabetes is not contagious. One human being carrying diabetes does not pass it sexually to another human being. In this country we have just been building up and building up and building up this huge population of people who are carrying the virus but are treated successfully, so they are living decent lives. And our death rate has plummeted, that’s fabulous. That is great news. I mean that’s really spectacular, and I have friends who have been living with HIV for more than 20 years, and are by all outward appearances remarkably healthy individuals-even healthier than their non-HIV peers. But that means that we have this huge population growing that does have a immuno-deficiency virus in their bodies that is transmissible, and also may put them in special risk should an epidemic or something else emerge in our society. If you compound this and imagine it in societies that have some access to drugs but only for the elite, only for the wealthy, but the greater masses have no access. Then you can see scenarios in which treatment itself can become a source of destabilization or even a motivator for civil war or for over turning government power. Why should we in the villages, why should we in the ghetto, all die of this disease, of a secondary assault of something else that comes in to our beleaguered immune systems on a mass level, while you the elite are on effective, anti-viral therapy and living happy, healthy lives and can sit and sip wine while the epidemic sweeps over our lives?
So what can we do? How can we combat HIV/ AIDS in these countries when treatment is not going to get out to them and when vaccines are a long way off?
I think in countries where HIV is being introduced through the needle, which is the case in some of the most populous nations in the world-it is certainly the case in parts of China, all of the former Soviet Union, Indonesia, much of Southeast Asia-there is a golden opportunity right now that could affect the whole historic course of this pandemic for the entire planet. And that is focused on the vector, the needle. Tremendous social and political change has to occur for these governments to feel right about reaching out to IV drug users as a public health concern for the community at large, in a non-punitive fashion.
Thailand shows us that rounding up all your drug users and throwing them in jail is not the solution. In fact, what happened in Thailand when they did that is it increased the spread, because all the guys in jail shared the same one or two needles, and by the time they got out of jail every one of them was universally infected. So it exacerbated their problem. So that’s number one from a historical perspective.
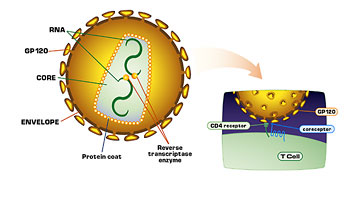
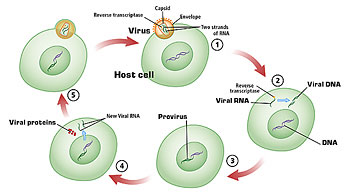
But in the parts of the world where HIV is really a sexual issue, there is no getting around it. I have thought this through for hundreds of hours. I have spoken to some of the most brilliant minds on this planet trying to understand where the answers are. And it really comes down to two things. We desperately need an effective vaccine. But we’re not going to have one anytime soon. There is nothing in the pipeline at this moment that looks, at the rudimentary level, like a good potential that could make its way through the whole testing apparatus and be available 15 years from now. So if we don’t even have anything in the pipeline now for 15 years from now, you can begin to see the scale of this problem.
We have never dealt with a retrovirus before. We’ve never imagined how to vaccinate against something that infects your DNA. We just don’t know how to do that. So barring some extraordinary breakthrough in science in the next few years, the answer comes down to a massive scale of social change. The question really is, can political leaders and powerful economic leaders take part-we’re talking at the G7 level, we are talking at the level of Bill Gates and colleagues. And Bill Gates does get it. He is the biggest private donor trying to deal with AIDS right now in the whole world. No one else comes close. But can Bill Gates’ colleagues, his friendly billionaires, can the heads of state all over the world get beyond rhetoric and stop just passing the occasional UN resolution, or creating a fund to which they give no money? Can they get to the point where they really are saying from the political pulpit and the religious pulpits with pressure, “People, we can’t play games anymore, you know this is not about wishing it will go away, or pretending that everybody’s individual lives will just go on as they were and you’ll be the lucky one that can roll the dice, day after day after day and not end up dying of AIDS.” We have to reconsider how men and women relate on this planet. We have to reconsider it completely.
[Note: Samora Machel became independent Mozambique’s first president in 1975 after leading the revolution to oust the Portuguese. He was killed in a somewhat mysterious airplane crash in 1986.]
I’ll give you a cogent anecdote that was a huge learning experience for me. I was only in my early 20’s; I was living in Africa. I had gone to Mozambique, which then was newly controlled after a couple of centuries of Portuguese colonialism. The leader was a man named Samora Machel, a very admired visionary figure in African history-he’s still much beloved by many Africans. Samora was trying to build this great new society, but he was hearing that in the absence of the brutality of colonialism, many old tribal laws were beginning to re-emerge in pockets of Mozambique and in particular, all of a sudden, a lot of women were being killed by their husbands in public settings: hung from trees in the middle of a village and so on. Old tribal laws said that if a man is dissatisfied with his wife, he may kill her and take a younger wife; that was an old tribal rule.
Machel realized he had to nip this in the bud. So he went out, and I was fortunate to be one of the journalists permitted to go with him, to a village in which there had been an extraordinary number of wife killings in a very short period of time. And here was the setting: all the women sitting in the periphery in terror with their children while the men were in the middle with Samora Machel arguing about, first and fundamentally, is a woman worth more or less than a cow? Now that argument took many hours, is a female human being of greater value than a cow? And Samora Machel had to say, “Well, does the cow wash your dishes, does the cow give you babies, does the cow raise your babies? Does the cow do all the farming in the fields? Because the men never ever farm since that is a woman’s job. Does the cow repair the roof on the house? Does the cow give you love and affection? Well, love and affection aren’t really an issue. All this arguing took many many hours until finally there was a breakthrough: “Yes, I guess a female Homo sapiens is worth more than your average bovine. Alright, now can you get to the point where she has the right to life, literally, and she has a right to say something. Do the women in this village have any right to vote over anything that may be in this village’s future?
You have to get beyond that point before you can stop this epidemic. And if you think I’m only talking about Africa, go take a look at what it’s like to be one of the women in the lower castes of India today, or to be a woman living a rural life in China today, or for that matter to be woman in the middle of Siberia today. We as American women have a very hard time imagining what it’s like for most women in this world right now. But this is a virus that has exploited very, very successfully the inability of most women to control their own sexuality. And my fear is that with most heads of state being men, most of the leadership of the world being men, my fear is that all this gets written off as feminist blather and by the time any head of state really actually comes out and says, “Fellow men, we can’t behave this way anymore,” I fear that by then they will have lost half their populations to this virus.
What can we do then? Just stand by and watch it happen?
No, I mean the most horrible thing for our society is to be a bunch of AIDS voyeurs, to all sit down and be death voyeurs, watching the occasional CNN special on whole villages devastated by this virus. Then, in your history class, you’ll have historical metaphors about the plague to compare it to. That is not a satisfactory answer. I think the kind of intellectual rigor that needs to be brought to this, with the appropriate sense of urgency, hasn’t happened yet. And you know we’re kind of willing to let a fairly cumbersome and largely ineffectual United Nations apparatus try to cope with it, along with a few foundations and a couple of humanitarian organizations. We haven’t really as a global community woken up and said just how serious this really is.
So the kind of action that needs to be taken to make some kind of change isn’t possible until first everybody really wakes up, stops being in denial, stops pretending it’s only somebody else’s problem, and says, “You know, we as a species are under threat. Let me just remind you. This is a brand new epidemic. It has only just begun. What we see now is roughly a cumulative 65 million people infected, 40 million living with it right now, 5 to 6 million newly infected every year. There is somewhere in the neighborhood of 14 to 18 million children left orphaned already by parents that died of this disease, with all the instability that creates in the economy and so on. This is nothing. This is just the beginning, people.
All I need to remind you of is that we’ve not yet seen a single human being with natural immunity to this virus. We’ve not yet seen a single person who is making antibodies that stop HIV.
What that says is, it’s a new virus to our species, and like all new viruses coming into a completely immuno-naive population, it socks the population, and slowly but surely, over time, some naturally immune people will emerge. There will be a selection process, a natural selection, a Darwinian action and those who are immune will survive, and that will be the future of humanity. Well, hello, we haven’t seen any of that yet. If you look at the chart, if you look at the official United Nations chart, deaths from HIV going up one side and years since the epidemic began, the chart number looks like this, it’s almost a 90 degree angle, right? Even with the invention of highly active retroviral therapy that has stopped this death rate in North America. Statistically, it has had no effect on the international deaths because statistically it’s not available.
Americans are a tiny percentage of the problem. What this says to us is that you have to take your imagination out of its current box. You have to be thinking not of 40 million people infected, or a 100 million people infected, you have to think, as the US Census Bureau has, of 6.4 million deaths a year in Africa alone-a place with only 360 million people. You have to be thinking of 25 to 40 million people a year dying of this disease. You have to be imagining what a 4% or 5% incidence of HIV in India with 1.3 billion people means. You know, if you’re teaching a math class, let’s give some kids some examples. What is 4% of 1.4 billion people? If the death rate is let’s say 1% a year, what’s 1% a year of 1.4 billion people dying of one disease? Then add on 1.2 billion Chinese. That’s the way we have to begin to imagine.
I think fundamentally the real hope lies with the younger generation of the planet today. All the teenagers on Earth and the pre-teens, as dreadful and horrifying as it may be getting them to actually imagine this epidemic, they have to think out of the box, ahead a decade, two decades, to the point where not only do they feel motivated to protect themselves but to protect their societies.