


















Rediscovering Biology: Molecular to Global Perspectives
Human Evolution Expert Interview Transcript: Kari Stefansson, M.D.
 CEO and Chairman of the Board, DeCode Genetics
CEO and Chairman of the Board, DeCode Genetics
CEO and the Chairman of the Board of DeCode Genetics in Iceland. The company takes advantage of 1,000 years of genealogical records kept by the Icelandic people, and of the willingness of Icelanders to make their DNA available to the company for study of genetic patterns in disease.
Interview Transcript
Kari Stefansson, M.D., is the CEO and the Chairman of the Board of DeCode Genetics in Iceland. The company takes advantage of 1,000 years of genealogical records kept by the Icelandic people, and of the willingness of Icelanders to make their DNA available to the company for study of genetic patterns in disease.
Can you define the term “population biology”?
What people are probably referring to with the term “population biology” is biology that started in the context of a particular population, where people are not focusing on individuals, but they’re focusing on the population in general. So what you’re looking at, when you’re looking at particular parameters of biological function, is that you’re looking at the averages, or you’re looking at what characterizes the population rather than the individual.
Population genetics is basically genetics of the particular traits, or characters, of man, in the case of human population genetics, that then pass between generations with a particular population. It describes the forces that influence the transmission of the characters from one generation to the next, and genetics is basically the study of the information that goes into the making of a man. This is of course an extraordinarily important discipline.
Genetics is basically the discipline, the study, of what is at the heart of the definition, or the line of distinction, between what is living and what is dead.
Genetics is the study of the information that is passed from one generation to the next, not only in the case of man, but of all living organisms. And at the heart of everything that is living is basically a bit of information. The bit of information is the most fundamental unit of all life, and what distinguishes the information that produces life from other information is the ability to replicate itself. So we’re basically talking in terms of the study of very fundamental and very important concepts when we’re talking about population genetics.
Can you define a single nucleotide polymorphism, or SNP?
An SNP is a single nucleotide polymorphism. Remember that the human genome is put together from A’s, C’s, G’s and T’s. The information that we were just talking about, this very important information, is put together from a four-letter code. An SNP is a place in the genome where, in some individuals, one nucleotide substitutes for another nucleotide in certain proportion of the population.
And why are these SNP’s important instruments? They’re important in and of themselves because they dictate variation in the genome that is then reflected in the various phenotypes of the population. The SNP’s are among the reasons that some of us have green eyes and other blue eyes, etc. But they’re also important as instruments. They’re important as instruments to help us to map genes. When you are trying to map a gene, one of the things you do is that you take a large number of regions where these variations of sequence, either SNP’s or bigger variations, like in the places that we call microsatellite.
And then you look at these variable regions, and you look at a large number of them, and you try to find the SNP where you have more than a chance association between one form of the SNP and the tendency to develop a disease. If you find such a correlation that is statistically significant, it is likely that a gene that you’re looking for is in the neighborhood. So this is the way in which you get to the neighborhood of a specific gene within the genome. Then, before you find the gene, you have considerable other work ahead of you.
What can looking at SNP’s and the human population tell us about evolution?
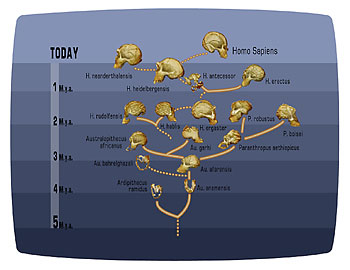
One of the things that you can do when you’re studying differences between populations is to look at variable regions for these SNPs and other genetic markers in various genes, and in the mitochondrial genome as well. And you can compare the population by comparing these SNP’s, or these genetic markers of variation in the various chromosomes or in the various genes. Then you can draw up basically a pedigree of human population-which one came first, which one is the most closely related to each other and so on.
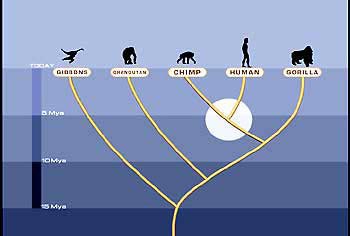
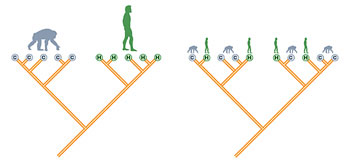
You can extend this study beyond that and you can begin to compare, for example, the same regions in man and in non-human primates. You can compare these between man and other species that are farther down in their phylogenetic tree. And you can gather substantial circumstantial evidence in support of a certain method whereby evolution has taken place.
Most of the studies that today make use of molecular genetics to look at evolution come to conclusions that cannot be directly proven because you cannot reproduce the experiment. We cannot reproduce evolution. So most of what we’re doing is collecting circumstantial evidence, the weight of which can become substantial when you look at large numbers of genes, look at a large number of species, you put us together into one big picture.
And what is the purpose of your company, Decode?
You see, Decode is a genetics company in Iceland that is focused on studying the genetics of common diseases in the Iceland population. And you have to realize that Iceland was inhabited, was settled, about 1,100 years ago. It was settled between the years 870 and 930 by people coming — men mostly from the west of Norway, and women coming mostly from the British Isles. Actually the Boca Settlement that was written 1,000 years ago said that Iceland was settled by Norwegian Vikings who stopped by Ireland and pick up slaves.
We have done a very large genetic anthropology study of Iceland, and we looked at mitochondrial polymorphisms to look at maternal lineage, and Y chromosome polymorphisms to look at paternal lineage, and we have come to the conclusion that about 70% of the Y chromosomes in Iceland have come from western Norway and about 70% of the Icelandic mitochondria are Celtic. So our genetic work has sort of validated the view of the Boca Settlement.
Since the country was settled, Icelanders have, for whatever reason, been very interested in the genealogies, and we have now, for example, in Decode, a little company, we have the genealogy of the entire nation going 1,100 years back in time on a computer database. And as you look at all the Icelandic records, all of them begin with a page after page after page of genealogy and we could spend a long time speculating on why Iceland was so obsessed with the genealogy, but the fact of the matter is that we have this.
And why is that important? It’s important because the study of human genetics is the study not only of the information that goes into making a man, but also of how this information is passed from one generation to the next, and the genealogy gives you the avenues by which this information is passed.
This is also important because this interest in genealogy is an expression of a much broader interest in the population, an interest in the history of the nation, and Iceland is passionately interested in their history, and they are very much interested in participating in telling a story.
And what we are basically doing at Decode is to take this old study that is basically written in the genealogy of the entire nation and add different chapters to it. The chapters are about certain vulnerabilities that are passed on from one generation to the next within these big families — and this is not only our view; this seems to be the view of the population in general because we have had enormously good participation rate in all of the studies that we have done.
What kind of participation rate are you talking about?
About 95% of people approached have participated in our studies, and I don’t have any numbers to compare that to, but to us, it looks like a very, very good participation rate.
What is the size of the Icelandic population?
The population of Iceland today is about 285,000 or so, and about 85,000 people have participated in our studies, after signing informed consent, have given us blood so as we can isolate DNA from it.
And, one of the big advantages of working in a nation like the Icelandic nation is that the size is so small that we can work with everyone who has a particular disease in Iceland, but it is sufficiently large to give us enough cases of basically all diseases that have prevalence that is greater than .2%.
Is this targeted disease approach unique?
I don’t think that our approach is in its very nature so different from others. There aren’t all that many ways in which you can do these things. But one of the things that we realized relatively early on is the necessity of finding ways to get around the fact that when you start a study of the genetics of our common diseases, there’s no way in which you can predict how much information you need to be able to map a gene before you start your work.
When you’re looking at the old, you know, relatively simple rare Mendelian disorders, you could calculate in advance how many people you needed to study, how many patients, to be able to solve the problem of the disease and to be able to map a gene, because you knew the relationship. There was 1:1 relationship. You have a mutation, you will develop a disease; you don’t have a mutation no you won’t.
In the case of the common diseases, this is much more complicated, and you cannot predict the amount of data you need to be able to map a gene. So we started out by putting a lot of emphasis on collecting vast amounts of data, both in the form of the number of patients, and the relationship between patients by genotyping or looking at many variable regions. We look at probably three times the number of markers that most people do when they are doing genome marker counts, and we have an advantage from a position where we are studying all of the diseases in the same population.
The reason that is important is that you gradually learn a lot about a population and every all the data you collect in the study of one disease is gonna benefit you in the study of the next disease, etc. So gradually, by mining always the same population, you begin to see a pattern that helps you to solve the parcel of all of the diseases that you are studying.
I think that what was possibly lost on many others working in the genetics of common disease before we started our work is that the key, the scarce resource, is the population because what you are studying is the information that is carried in the people. You’re studying information that is reflected. First of all, it is encoded in the A’s, C’s G’s and T’s, and in the genome of these people, and it’s reflected in who these people are when it comes to the strength and the vulnerabilities. They are the key. You’re not going to solve the parcel of the genetics of any disease by lining up a large number of DNA sequences. I mean you can’t just go to the store and buy them.
What you need is a population that you understand, that is willing to work with you, and that has a significant amount of information about the relationship pattern that dictates how information has been passed. This is the scarce resource and we were so fortunate, first of all, to realize this, and secondly to be able to find the population that had all of these qualities just by opening the door to our house.
How have techniques changed the way you look at population genetics?
What is particularly useful, of course, is to have the sequence of the human genome because although the sequence of the human genome is only the sequence of the reference person, it gives you sort of the outer boundaries of what you need to look at. It diminishes the necessity of having to do a lot of sequencing yourself. It is enormously enabling.
Number two, the DNA sequences have allowed us to do genotyping, which is what it is called when you’re looking at these valuable regions, with a speed that was unknown 20 years ago. You see at Decode, we can generate up to 50 million genotypes a month, which is an enormous amount of genotypes by using the instruments that we have.
But the most important instruments are, however, not the DNA sequences but the software systems we have that allow us to collect, store, and analyze the data very quickly, and these are software systems that have been written by our own people-software systems of the sort that were not available 10-20 years ago.
And then it is the great equalizer, the computer. Computers of the type that we have today didn’t exist 20 years ago, and computing power is at the heart of being able to utilize large amounts of data in their analysis of this ever so complicated relationship between variation in the sequence of the genome, and the tendency to develop a disease, or the ability to resist the same disease.
Can you explain what you mean when you say you’ve created a “high-resolution genetic map”?
The sequence of this human genome was only a sequence of the referenced genome. And if you look at it alone, you could get the impression that the genome is some static thing that doesn’t change. But the fact of the matter is that every time an individual is born, every time a child is born, an individual has been created for the unique genome, not only because the individual gets half of his genome from the mother and half from the father, but also because in the generation of germ cells, recombinations take place. There is an exchange between chromosomes. And the recombination is at the heart of the individual’s relational variability in the sequence of the genome.
And when we put together this genetic map that has a resolution that is substantially greater than any such map that has been generated before, we saw a lot of new, very interesting things, and some old observations were reinforced.
And one of them is that the combination rate is very different between men and women. Women recombine 1.6 times more frequently than men. They have peaks of recombination, or recombination hot spots, that are different from men, so there are some places where there is a lot of recombination in women and much less so with men.
It doesn’t take a geneticist to see that there are differences between men and women-thank God. But there are some differences that we have been picking up that indicate that the role of men and women, when it comes to evolution, are possibly a little it different.
When we took advantage of this enormous strength that lies in having the genealogy of the entire nation, we could basically begin to look at all of the people who participated in our high density genotyping, which went into putting together the map. And we saw that there was a difference between families when it came to recombination rate. Some families have a high recombination rate; other families have a low recombination rate.
And even more interesting, we can see that if you looked at women, that women who recombined a lot had many more children than women who recombined little. So when you put that together with all the data that exist out there, we gradually sort of came to the conclusion that the recombination might actually be a prerequisite for procreation; that without recombining, man would not be able to generate offspring.
This is interesting because, in the context of the study of the genetics of disease, there is a fairly good correlation between the places where you have a high density of genes, where you have significant nucleotide variability, where you have recombinations, and where you have mutations.
So basically one of the prerequisites for being able to generate offspring is to recombine at the high rate in regions where you expect that you will have mutations, so the only way to live is to live dangerously. You’re not gonna live unless you participate in a process that has a fairly high risk associated with it.
But these are all interesting things. One of the things that has come out of this genetic map is that now you have a fairly actuate placement of these variable regions, these markers, that allow you much more accurately to map genes and diseases, and what’s more, it gives you the opportunity to look at it in a sex-specific manner. Because it is clear that, if you are going to take full advantage of what the technology to map genes gives you, then you have to look at it in a sex-specific manner because of the differences in the recombination rate between men and women. They’re not only different when it comes to their recombination rate, but also their locations.
Can you cite some examples of disease-causing genes?
I can give you examples of genes that interest me in particular. I can give you examples that interest me personally, although I think that all of them are interesting from the point of view of understanding man in general.
The one that I find particularly interesting is this schizophrenia gene that we have recently isolated. Schizophrenia is probably one of the most feared diseases of man. It is a disease of the brain as an organ of consciousness, and the brain as an organ of consciousness is the organ that separates man from other species, so this is a particularly human disease. And it has turned out to be very, very difficult to establish any sort of foothold in the biology of schizophrenia, and there have been a number of false leads that have come up over the past five to 50 years.
The gene that we have isolated in schizophrenia is a gene that makes a protein that is called neuregulin, and it is particularly interesting in the sense that it’s a protein that stimulates the formation of synapses, and synapses are the places where neurons talk to each other.
And not only does neuregulin stimulate the formation of synapses, it also stimulates synaptic plasticity. One of the principal ways in which the brain responds to experience, responds to the environment, is by re-forming synapses through synaptic plasticity, or change.
And why is this particularly interesting in the case of schizophrenia? It’s interesting because schizophrenia has both a genetic and an environmental component. The genetic component is reflected in the gene that makes neuregulin. And since one of the fundamental ways in which the brain responds to experience is through synaptic remodeling, it is possible that the abnormal way in which the schizophrenic brain responds to the environment is actually initiated through the protein made by the same gene.
So this is actually a gene that may give us an explanation not only for the genetic component but also for the environmental component, so the old debate, “is it nature or nurture?” in the case of schizophrenia might be a debate on really nothing, because it’s one and the same thing, really.
Schizophrenia is also an interesting example from my point of view because it is also the first disease where we have isolated the gene and it has led to the development of a screening program within our company, on the basis of a discovery of a gene.
Another example I can give you that I think is particularly interesting is an example of our work on the genetics of rheumatoid arthritis and osteoarthritis. This basically shows you that what looks on the surface as being very, very complex genetics of a common disease may gradually be teased into relatively simple genetics or the vulnerability of an organ or an organ system.
We mapped rheumatoid arthritis to a gene in the major histo-compatibility region. And there’s a very, very tight association between a variant of one of the histo-compatibility genes of rheumatoid arthritis called DF4, and 60% of our patients are DF4 positive. If you take out the 60% of patients and we reexamine our data just on that 60% of our cohort, we find another gene on Chromosome 3, and it happens to be the very same gene that is also associated with osteoarthritis which is a degenerative disease of joints.
So here you have a situation where there’s both a variant in one gene and another factor on a chromosome. So if you have one alone, you may develop osteoarthritis at a relatively late date. However, if you have the variant of this gene and you’re DF4 positive, you will develop rheumatoid arthritis at a very early age. So this gene on chromosome 3 seems to confer a general vulnerability of the joint, not the specific disease.
So the more you study and the more you look, the more integrated this world seems to be, and the more convinced you are that these very complex biological pathways seem to be coming together to form an individual. This is all interwoven into one cloth. And basically, before we can manage diseases fully, completely, as well as theoretically possible, we have to develop some sort of an overall view of man. We have to understand not only individual biological pathways but also how they are integrated into forming this very strange creature.
Can you outline the steps you took in isolating the schizophrenia gene?
The way in which we isolated the schizophrenia gene was to gather a list of patients with schizophrenia in Iceland, and that was done by a psychiatrist who was taking care of the patients. And then the list was cross-referenced with a genealogy database that covers the entire nation, and out came family trees. This patient list, when we got them into the company, had only encrypted ID’s to protect the privacy of the patient.
So, out came family trees with encrypted ID’s, and our statisticians collected the patients that they thought would give us the genetic power to map the gene. We sent it back to our psychiatrists whom we were cooperating with, and they send out letters to patients and their relatives and asked whether they would be willing to participate in the study.
This is somewhat difficult in the case of a disease that influences the brain, a disease that deprives people of clarity of thought, of contact with reality, so the schizophrenia study was particularly difficult when it comes to this. And it’s always a question when you’re dealing with a psychiatric disease: who is it that should give the informed consent? Should it be the patient? Should it be relatives? Are you entitled to deprive the patient of the right for self-determination, just because the patient has a psychiatric disease? And in most instances, you go to the patient, because he has the right to make the decision–in most instances–in spite of having some thought disorders.
But anyway, we and our collaborators, the psychiatrists, spent an enormous amount of energy trying to figure out the right way of doing this or the way that sounded right to them and to the patients.
Once we had collected enough material, enough blood from enough patients, we isolated the DNA and then we did the genotyping. The genotyping is done by looking at, in our case, about 1,100 variable regions in the genome. Eleven hundred of these microsatellite markers. These are, in this case, not SNP’s, not single nucleotide polymorphisms, but bigger polymorphisms that have more information value.
Once we had done this we used linkage, which is a family-based method, to look at segments of DNA that are yet to be affected in members of the family. We established linkage to Chromosome 8. There’s a region on Chromosome 8 that had a very, very high signal.
Once we did that, we took this region and we increased a number of markers in that region dramatically, so we got much more information out of it, and that pointed us to a relatively small region, and from that region we took an even higher density of markers, and by stringing together several markers into what is called a haplotype, we could demonstrate that there was a very, very tight association-far above what you would expect to see by chance alone. The “p” value, which is a measure of the probability of finding this out by chance alone, was vanishingly small, and we could demonstrate that this haplotype that contains seven markers was within a small region of a very large gene that makes the neuregulin.
This is the fundamental method that we used. Then, once we had done this in the Icelandic population, we went to a Scottish population and demonstrated that the same thing applied there.
Then the question comes up, how do you take it beyond this to look at the biology of this? Yes, indeed, we looked at knockout mice where the neuregulin gene had been knocked out, and another set of mice where the receptor for the neuregulin had been knocked out, and these mice demonstrated behavior abnormalities. They had increased open-field behavior: movements in an open field were much greater than in the control mice.
And they also showed the loss of what is called “pre-pulse inhibition,” which is characteristic for schizophrenics. This does not mean that the mice had schizophrenia. Schizophrenia is a disease of the brain as an organ of consciousness and the consciousness of men and mice differ a little bit, and I think it would be difficult for a mouse to become schizophrenic.
But these changes are in keeping with what you see in animal models with schizophrenia, in keeping with what you see when mice have had angel dust or PCP, which is one of the ways in which people generate animal models for schizophrenia.
This animal model, or this mouse model, is important because not only does it shed light on the role of neuregulin and behavior. It also generates reagents for you to use when you begin to start [drug] development. So this is basically in broad strokes what we have done with schizophrenia.
How does one detect genetic variation?
If you would take DNA from me and you would take DNA from you, we would sequence our genomes, it would take considerable time to figure out the meaning of the sequence differences that we would see. It wouldn’t take more than a fraction of a second to look at me and you to see that there are meaningful differences between the two of us.
So in spite of everything we have learned about the nature of the genome and the importance of certain aspects of the genome, we are far cry from being able to assess in a meaningful manner the sort of implications of what may lie in differences in sequences between various ethnic groups. It is much easier for us to understand each other as human beings by talking to each other than by looking at the sequence of our genomes.
It is also absolutely clear when you travel a lot like I do and you talk to people in the various countries of this world that there is a dramatic difference, a dramatic variation of the phenotype within a population. There is hardly a place I have been to where I have not found people I like very much and people I don’t like all that much. So there is a dramatic variation within these ethnic groups that is probably much greater than the differences between groups in the populations.
And I think that you’re going to find the same when you look at the variations of the sequence. Indeed, there are variations between groups, between ethnic groups, between nations. But these average differences between the groups are probably much less than what the variations that you see within these populations.
So I think that if you want to learn, if you want to understand or try to understand the differences between various ethnic groups and nations, read the literature, listen to the music, talk to the people. Don’t look at the sequences. It’s not gonna tell you all that much.
What utility do you see in mitochondrial DNA?
The mitochondrial DNA is very useful when you begin to look at old samples, when you look the skeletons and you try to use genetics to understand the evolution of a population, because there are so many copies of the mitochondrial genome around because each cell has so many mitochondria but only one nucleus.
We have spent substantial energy in looking at the sort of genetic anthropology of Icelanders because we are working always with Icelandic population and we want to understand it as much as we can. And by combining the vast amount of information in the genealogy that we have with the mitochondrial stuff we have learned a lot about Icelandic nation.
It doesn’t help us all that much in our disease world to look at the mitochondrial DNA because the mitochondrial diseases are few, and they are not among the common diseases of man, which is what interests us the most. But it has certainly given us a lot of fascinating information on the evolution of the Icelandic population.
How exactly can this data be used in drug development?
Drug development never does move swiftly and there are all kinds of reasons for that, scientific, technical, and societal, and the societal reasons are probably of the greatest importance, because as a society we are always elevating the bar when it comes to conditions, when it comes to demand for safety, etc., when it comes to drugs.
And the average time it takes to develop drugs today based on a basic science discovery, like a discovery of a gene, is at least ten years. So there is going to be some waiting before the first drug comes from my work that is based solely on the discovery of a gene.
And keep in mind that almost all of the therapeutic expectations that we have is for classical drugs. You’re not talking in terms of gene therapy, which is something that I do not expect is going to have a significant influence on our healthcare system for at least ten to 25 years.
But we are sort of in sync towards drugs on the market based on gene discovery. We have programs in our company now in about five diseases based on genes that we have discovered. And we are working with very good drug targets that have come out of the gene discovery, and we certainly hope that, with those, we will be able to thump our chest and say that we have contributed to alleviating suffering by discovering genes.
There are going to be diagnostics on the market substantially sooner because it doesn’t take all that long time to develop diagnostics. Keep in mind that good diagnostics have always to precede good treatment, because you have to be able to diagnose accurately before you can begin to develop drugs that are very effective.
How would you answer critics of your company that say that you are abusing the rights of your participants?
It is an important question, of how you use information about people, and how we approach people, how you protect the privacy, how you watch over their interests; all of this is extraordinarily important when you’re doing biomedical research. And when you’re working on human genetics, you’re working with the information that goes into the making of a man, and I think that this information comes as close to being sacred as any information. So you shouldn’t treat it in a frivolous manner. You should treat it with respect, and you should do your best to make sure that it is only used for good.
But there are so many colliding views when it comes to how one should study the biology or the genetics of diseases. But when you sit down and talk to patients, when you talk to their families, when you talk to the people whom the diseases are touching at this very moment, the concern is not privacy. Their concern is not that people are hurrying too much when it comes to the study of the nature of the disease. Their concern is that we are not doing it fast enough, that we are not putting enough emphasis on this.
And I can tell you that in Iceland we are held to an extraordinarily high standard when it comes to the protection of privacy in our genetics research. All data that come into our company are, for example, with encrypted IDs — encrypted by a third party.
And I can tell you the first thing that patients complain about when patient organizations come and visit us is this third party encryption system. They insist that it is their right to interact personally with the scientist, because they believe they can motivate them, they can help them, they can stimulate them and they insist that this heavy emphasis on protection of privacy is not watching over their interest that is watching over interest of some subculture in society that is for whatever reason obsessed with privacy. Whether that is true or not, I don’t know.
But if you think about it, if you ask the question: When I go to a hospital, what is it that I am using? What resources am I using when I visit the healthcare system? What you’re first and foremost doing is that you’re using experience; you’re using knowledge that was discovered because the people who came before you to this very same healthcare system allowed the information about themselves to be used to discover new knowledge to advance medicine.
And I think that the case could be made that it is your obligation to allow the information about you to be used so your children and their children will have access to an equally good healthcare system in the future. I think that our right to use the healthcare system, which is the product of the fact that others allowed the information about themselves to be used, comes with an obligation of allowing the same information about you to be used for the same purpose.
This is a view that is based on my sort of conviction that your rights in society come with obligations but not everyone sees that view with me.
So do you see most of the benefits of this research as being for future generations, rather than for us today?
Given the best-case scenario, when we have discovered the gene that turns out to be truly the gene that causes the disease, it’s gonna take at least ten years, if not 15 years, to turn it into drugs on the shelves. So it is likely when we are dealing with serious diseases that the people who have donated DNA, who have participated in the studies are not going to be the primary beneficiaries, but it will be the patients of the coming generations. But that’s always so.
What does this research hint at in terms of future evolution of man?
I have absolutely no thoughts on how man is going to evolve. I have no speculations. I have no desire to know it. I am sufficiently deeply into studies of what has happened to evolution that has already taken place.
One thing, however, I think is important to recognize when we’re talking about human disease, when we’re talking about the genetics of common diseases is that we probably will never get rid of them. And why is that? Because the common diseases, most of them are caused by variants of so many genes, genes that when they are separate from the other genes contribute to human diversity, and I think that if you take all of these disease genes, and if you said to yourself I’m gonna develop some kind of a magic gun that allows me to blast away all of these bad forms of these genes you would probably get rid of man because I think that most of these common diseases have to be looked upon as an expression of the limitation in the design of man. Because, although man is a pretty interesting animal, we certainly have our limitations, and we are born into this world to die, eventually. I mean that’s part of the deal, and these disease genes probably contribute towards bringing us to that end, which is to make space for those who come after us.
What do you most want people to understand about human genetics?
If you think about genetics, and you think about the human genome and what a human genome does, my guess is that, for all the wrong reasons, there have been some societal pressures against starting the genetics of some aspects of human behavior, which is human nature, because somehow people seem to be concerned that discovering more about these aspects of man will somehow lead to some sort of a bad behavior on the behalf of society.
But I think that in this case, we will start a genetics war of sorts, because it is inherent to man to try to learn more about himself, which has to do with his intellect.
And I think that the acceptance of doing this has been growing of late, and I think that within a few years we will have spent considerable energy on questions of that sort, because that’s the only way I think that we will eventually understand the function of the brain as an organ of consciousness, which is the ultimate gold standard in the study of human nature. And I think that we will do that. I think that we will allow ourselves the luxury of understanding ourselves a little bit more.
What particular questions interest you most?
The questions that interest me. I am, you know, just running a little genetics company up in Iceland. I have a passionate interest in figuring out how we, for example, take a gene that we have recently discovered in myocardial disease, and in a calculated fashion turn it into drugs on the shelf. It is a disease that kills 30% of mankind and I believe that we have certain ideas that are going to bring us towards a drug in that case relatively swiftly.
I am waiting with bated breath to see them eventually pull out a gene in asthma. We have mapped several genes to genome significance in asthma, and we have our hands on the tail of these genes, and I look forward to seeing exactly what they are.
I’m interested in these little questions. There are a lot of people with big questions. But I have smaller questions, and I want to see them answered.