




Rediscovering Biology: Molecular to Global Perspectives
Emerging Infectious Diseases Expert Interview Transcript: Rita Colwell, Ph.D.
 Marine Microbiologist
Marine Microbiologist
Dr. Colwell is a Marine Microbiologist and serves at the President of the National Science Foundation. She is an advocate of an integrated approach to studying disease called biocomplexity, giving a holistic, system-wide view of the causation and effects of disease. She was pioneer in the research done on the Cholera epidemics in Bangladesh. She was able to help define causation and drastically reduce disease in the communities through public health education.
Interview Transcript
Dr. Colwell is a Marine Microbiologist and serves at the President of the National Science Foundation. She is an advocate of an integrated approach to studying disease called biocomplexity, giving a holistic, system-wide view of the causation and effects of disease. She was pioneer in the research done on the Cholera epidemics in Bangladesh. She was able to help define causation and drastically reduce disease in the communities through public health education.
Tell me what biocomplexity is, and how it’s affecting the way we think about diseases?
Historically, as scientists, we have taken a highly reductionistic approach to understanding life. We’ve looked at molecules, enzymes, atomic structure, sort of drilling down finer and finer.
But we’re finding now that we really need to understand life holistically, not just the electron structure, the molecule, the organism, but also in context of a community, populations in the environment in total. Again, we’ve also learned that we cannot deal only with a given region-we find that in the case of infectious diseases, it’s continental and intercontinental, therefore we really need to take a global view of interactions of microorganisms with humans in the environment.
This hasn’t been possible up until now because we haven’t had the capacity for handling huge amounts of data, which we now have. We have electronic computers; high-speed computers with the kind of high-end computing that allow us to search massive databases. So the epidemiology that has developed, the data that’s been accumulated in other countries can be merged with the data that we develop here in the United States so we can get a global picture of epidemics, of AIDS, malaria, yellow fever, dengue, cholera, influenza.
So it provides us with a hugely powerful new dimensional perspective for looking at infectious disease, looking at health, and looking at our interaction with our environment.
Does biocomplexity mean that you look at everything as a whole instead of tearing it apart individually?
Biocomplexity really incorporates all information, the atomic, the organismal, community structure, population, and global. That is, it integrates all of the information that gives us a holistic view of the system as opposed to just one small component of it.
So biocomplexity gives us an entirely new way of looking at the environment, our interactions with the environment, especially something as complicated as infectious disease.
In the past we were really focused on the pathogen and the human, the host, or in the case of agricultural diseases, plants and animals. We felt that it was a direct interaction, whereas we now know that it’s much more complicated. We have found that most diseases actually have a seasonal incidence. For example, diarrheal diseases have been known to be highest in the summer months, influenza highest in winter months. The assumption has been, well, it’s simply the fact that there’s more pollution. In the summer, we tend to drink water that may have more bacteria in it. In the case of influenza, we’re crowded in rooms and therefore we have more person-to-person contact. They’re rather simplistic, maybe not necessarily fallacious, but simplistic explanations of the infectious disease.
But now we understand that in fact cold viruses may have a predilection for the tissues of the nasal passages when the temperature’s somewhat lower as it is in winter months, hence the winter months may be a time when we have greater risk for cold virus infections.
We’ve been able to correlate the incidents of other diseases as well. For example, cholera in developing countries, particularly Bangladesh, the number of cases is much higher in the spring and much higher in the fall, and because we had traced the bacterium to an association with plankton and we know that plankton numbers are highest, the “blooms” as it’s referred to, occur in the spring and in the fall so that that provided us an opportunity to see the seasonal correlation.
Is it looked at now because the science has caught up with us to think that way?
It’s a convergence of having the tools of molecular biology, which are very precise in allowing us to detect the presence of, let’s say bacteria in water systems, where before we had to depend on culture and it was cumbersome. It took weeks. It was not as precise as we would like.
But now, we are able to pinpoint the genes and to say exactly what you have collected. Being able to do that coupled with the ability to handle huge amounts of data allows us to scan from satellites, see surface temperature, chlorophyll distribution, which precedes disease because of plankton carrying chlorophyll precedes the zooplankton blooms with which we know now from our long years of study how the cholera bacterium is associated.
Being able to pull all this together has been enormously exciting, has given us a fresh new view of microorganisms and of our role in the ecosystem, and again we are but another component in this ecosystem on planet Earth. But being able to portray it very precisely has been enormously reassuring and invigorating for the research.
What are the ramifications of ‘thinking big’ like this?
What this allows us to do now is be able to build a predictive capacity and to determine those factors, those environmental factors, climate factors, human population distributions, and to develop a prediction by computers saying, “Look, we’ve been measuring by satellite the sea surface temperature. We note that by measuring the temperature, chlorophyll populations, salinity, and a variety of factors, that predicting a cholera epidemic is possible.” So then we can do an alert, as we did in the case of Peru, we can have a boil-water alert-we can say, “boil your water, because the possibility of cholera outbreaks is very high right now.”
Now we haven’t been able to do that before — to really predict epidemics. We’ve been able to predict by taking historical data, developing patterns and say, “Okay, we think based on this previous data that this is going to be a time when we’ll have the influenza epidemic, and it is probably going to be this type.” But now we have reached a point where we can actually focus on the conditions and say, “Look, now we know these conditions are really conducive to an outbreak, and so let’s take preventive action.”
Now this has tremendous ramifications for public health costs, being able to carry out public health measures at the routine level but then go for a push when we know the conditions are right for an epidemic. So instead of having to be at high alert 24 hours a day, 7 days a week, 12 months a year, we can now pinpoint the alerts and be able to use our resources most effectively and efficiently.
Is it feasible, though, economically with poor countries, to be able to coordinate all this? How can we do that?
Countries like Bangladesh suffer drastic epidemics of cholera and other diseases, but cholera in particular. A few years ago during a time of severe flooding there were thousands of cholera victims entering the hospital in Dacha, Bangladesh, every day, and hundreds of thousands of victims over this short period of time.
Now if we can institute a recommended preventive measure, for example, being very careful to filter the water, being very careful to treat perhaps with chlorine at that particular time, we can abate the epidemic very significantly.
In countries like Peru, where there is enough fuel, enough electricity to be able to boil water, we can institute a boil water alert as was done during the epidemics in 1991-1992. We can post signs on billboards saying, “Cholera threat, boil water” so people will take extra precautions and get through that period of high risk.
It’s a matter of simply alerting the public, educating the public, and having the public take its health into its own hands. It can control to a certain degree its exposure, its risk to infectious disease.
How did you get involved in cholera research?
Well, I’ve always been interested in public health and medicine, and at one point, I pursued a degree in medicine but then I decided to go into research. I was actually working in marine microbiology at the University of Washington. I became very interested in a group of microorganisms that are found widely distributed in the oceans and in coastal waters. These are Vibrio bacteria. They’re tiny, microscopic, slightly curved bacterial cells that are widely distributed found in the guts of fish, cause disease of fish, but also as it turns out cause diseases in humans.
Now it was well known back in the 1950s that certain vibrios, like Vibrio parahaemolyticus — a fancy name for a bacterium that is associated with fish and shellfish-was a major cause and remains a major cause of illness transmitted by eating improperly cooked seafood.
It was not understood nor accepted that Vibrio cholera was in the environment. It was believed quite strongly that it was transmitted from person to person, and that any suggestions that it was in the environment was only that, oh, well, it was discharged by victims through the illness of diarrhea and vomiting into contaminated systems.
But we very laboriously showed over a 20-year period that Vibrio cholera is a normal inhabitant of coastal waters, estuaries, river systems and even fresh water where there’s a high calcium or magnesium content.
It was clear to us that the real cholera is a natural inhabitant in water systems. What we discovered was that between epidemics, it goes into a kind of dormant stage and it can’t be cultured readily. And so for years physicians and microbiologists working on cholera had tried to isolate the vibrio from sheep and from cows and from dogs and chickens and from water systems and soil, and they couldn’t do it between epidemics. During a massive epidemic, they could pick it up in the water because of the amount of pollution that had occurred.
So the assumption was, well, it doesn’t exist in the environment. It is passed from person to person. However, we were able to show with molecular genetic tools, using highly sensitive antibodies labeled with a color molecule, that we could see it under the microscope between epidemics in the water system, and using gene probes we were able to prove that it is present. We were able to show that it’s present in very large numbers. So with careful studies we showed that it naturally occurs in plankton just as we carry in our gut certain bacteria that really help us. Some of the bacteria produce vitamins that we need.
So there must be some function of these bacteria in the gut of this plankton, this zooplankton. They’re cocopods, tiny crustaceans.
And this association is very important, because the vibrios break down the strong white shell of crabs and the cocopods. It’s made up of chitin. All vibrios, including Vibrio cholerae, have a very powerful chitinase, an enzyme that breaks down that shell structure, so it plays a role in nature. If we didn’t have these vibrios in the environment, our bays and estuaries would be solid with crab shells and cocopod crusts, so to speak.
So the bacteria play a role in the environment, they’re present in the environment, they’re part of the natural flora, and we suspect that the toxins that they produce in the case of Vibrio cholerae probably play a role in nature that is not related to illness in humans. We suspect that the toxins of Vibrio cholerae probably play a role in osmoregulation, the ability of crabs and cocopods to migrate through very, very strongly changing water salinities, from very fresh water in the Chesapeake Bay near Baltimore all the way to full strength seawater off the coast of Maryland, and we know that crabs migrate from the open ocean all the way up into Baltimore, so we know that the copepods similarly are distributed. So coming back to biocomplexity, relationships that are seemingly unrelated to the infectious disease play a role in this spiral going from the sub-molecular to the molecular to the organismic to populations of copepods because it turns out that a single copepod can carry as many as 10,000 Vibrio bacteria.
And from studies done 25 years ago by other investigators using studies with human volunteers, it was determined that about a hundred thousand to a million bacteria per milliliter would be an infectious dose.
So now if you have a copepod bloom where one copepod can carry 10,000 bacteria, and if you maybe have a hundred copepods instead of one in the cup of water that you drink or maybe a thousand, you’ve now got an infectious dose. So this all fits together with population size, and then the massive epidemics that occur from people who drink untreated water as they do in Bangladesh and as they do in many other developing countries, in Latin America, in other countries, we then have the makings of a massive epidemic.
Did you discover that there were two peaks to the cholera outbreaks with the sea surface temperatures?
The serendipitous and the delightful discovery was that cholera seasons had been recorded for at least a hundred years, and in the last 50 years the seasonality of cholera had been well documented. A spring epidemic in Bangladesh was followed by a much larger epidemic in the fall-September, October, and November.
We had correlated this with zooplankton populations because we knew from our studies that the populations are higher in the spring and the fall and we thought, well, you know, we could monitor this by satellite thinking that we can measure chlorophyll by satellite. The chlorophyll bloom would precede the zooplankton blooms and we would figure the cholera epidemics would then come.
What we discovered by measuring sea surface temperature was that there was a remarkable peak in the spring, a dip, and then another peak in the fall, so we got a marvelous clue to the stimulus to cholera epidemics with a sea surface temperature warming leading to the bloom of phyto-plankton, which we measured by chlorophyll leading to the bloom in zooplankton which we could measure by doing counts in the water. And then we found that, sure enough, four to six weeks later the cholera epidemics occurred. And so that sequence of events is related and is predictable.
This was a wonderful discovery that really firmed up this very complex biocomplexity spiral going from molecular genetics to understanding numbers of bacteria, the interactions with other kinds of organisms in the environment and ultimately infecting humans and on a massive scale using satellite imagery.
Is biocomplexity applicable to other diseases too?
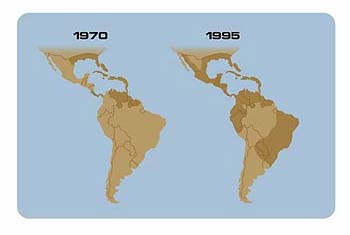
We find that there’s a pattern amongst the vector-borne diseases: Lyme disease, dengue, yellow fever, and malaria. There is seasonality. There is an association with temperature, with the climate, and a pattern of incidents that can now be predicted, and this relationship is critical, because if in fact there is climate change, if in fact we are undergoing global warming, we will then see a spread, geographically, for areas where there will be malaria that there hadn’t been.
Hanta virus is again a wonderful example of biocomplexity, because this disease broke out in the four corners where four states intersect, in the Southwest. It was a disease that hadn’t been met before, hadn’t been recognized, and it was killing young people via a respiratory infection.
Well, it turned out that the National Science Foundation had funded studies of mouse populations-deer mice-and it turned out that there was a correlation that was detected between the incidence of very high populations of deer mice, which was associated as it turned out with wet seasons, with the amount of food for the mice increasing-and thus the mice populations increasing-and then when there was a reversion to a less wet season, subsequently, these populations of mice went into barns and other dwellings to seek food. The virus that they carry, the hanta virus, is excreted in the urine. The urine dries in the dust, and then a victim comes into the barn, sweeps up the barn, inhales the dust carrying the virus, and comes down with this rapidly fulminating and often lethal viral infection.
So here’s another example of the complexity, virulence, the environment, the microorganism, in this case, the virus, and the populations of mice, the food supply, and seasonality all play a role in explaining this very complex interaction.
Does something tip the balance for these diseases to emerge?
It’s very, very important to understand that there’s a very important balance, a dynamic equilibrium between host, pathogen, the environment, factors that all together allow a very precise knife-edge balancing of all these factors. And then when there’s a tipping by let’s say a major weather event; then you have a disequilibrium, a reestablishment of a new equilibrium, to take from chemistry, and then you find diseases emerge or become ascendant. Something might tip the balance in favor of a very large replication population increase of let’s say the pathogen or its host, or its carrier in the case of mosquitoes and malaria.
Now epidemiology has been taught classically as tracking the disease, locating it, controlling it, and those are essentially the major aspects of it. We find that epidemiology is really much more complicated. It’s a subset of ecology, understanding the disease in terms of its environment, in terms of the climate, in terms of weather patterns. It’s a very complicated set of interactions.
How do you study biocomplexity? What all has to come into play?
The study of biocomplexity means that we have to move into the area of science that has become so productive right now, multi-disciplinary interactions. In order to study infections, it is not enough simply to study the medical aspects, the symptoms, the disease pathway, and treating the disease by an antibiotic or whatever the measures may be.
It means that we now need to understand through oceanography, space science using satellites to the best advantage, limnology, understanding rivers, streams, and so forth, microbiology understanding microorganisms especially in a time of bioterrorism reemerging/emerging infectious disease, clinical medicine, and epidemiology, ecology, systems ecology, computer science and so on, in order to be able to handle the data and modeling, which is an interaction with engineering.
So we find that it takes multidisciplinary interface between disciplines that the exciting new concepts, the new predictions, the new understanding and control of infectious disease will come.
So how would you now define biocomplexity?
Biocomplexity gives us the armor that we need to survive in a world that will never be free of or never have eradicated the agents of infectious disease. It’s not feasible to eradicate every microorganism that causes diseases in humans. First of all, there are what are called “opportunistic pathogens,” those that will infect and cause disease in an individual who is weakened because of other illness or because of malnutrition, etc., that are not normally considered to be pathogens. That’s one problem.
The other is that to eradicate major disease-causing microorganisms simply on a global scale is just not financially or biologically possible. So we have to understand these interactions. We have to be able to predict, and therefore to prevent. You might say biocomplexity is the science of survival.
What were the ramifications of your cholera study, and how did you help the people who were suffering?
When we had put together the information about cholera — and of course having worked in Bangladesh for more than 25 years — it occurred to us that we should use this knowledge in a very practical way to help the people of Bangladesh. Obviously the best thing to do would be to institute safe water supplies, centrally located and controlled, and sewage treatment, but that’s just not feasible in terms of the economics in the rural villages.
So we used our information to device a hypothesis. The hypothesis was: If the cocopods are the carriers, the vectors if you will, of cholera, if we could just remove them from the water we could reduce cholera. We wouldn’t eliminate it, but we could reduce the severity of the disease, because Richard Cash at Harvard University some years ago had shown that there is a correlation between the intensity of disease and the numbers of organisms ingested.
We tested this hypothesis first in the laboratory by thinking, “well, what kinds of filters could we use that everybody could afford, something that anyone could have?” We thought, “well — cloth.” So we tested the T-shirt material that men wear in Bangladesh. We tested Chinese poplin. We tested sari cloth. We found that if we folded sari cloth about eight times that we achieved a 20-micron pore size, and we know that cocopods are 200 microns, so we should entrap them, and sure enough when we did the experiments we found that we reduced the number of cholera bacteria 99%.
We reduced the number of cholera bacteria in the water by 99%. So then we proposed a study, which we carried out, a three-year study, where we brought together social scientists in a preliminary study because we were criticized in the review of the proposal to do this study that men would not drink water that had been filtered using sari cloth-old sari cloth, because we wanted to use inexpensive material-that had been worn by a woman.
Well, as it turned out, sari cloth had been used-single sari cloth-to filter flies from soft drinks. We knew then it would be accepted. We did a small pilot study. We found that we got well over 90% acceptance. So we then launched the full study.
We engaged workers-women-who went to villages every two weeks, to explain the purpose of filtering, explained how to filter, monitored the filtering and we located our test villages such that they were all equidistant from the hospital so that we could remove all of the variables that we possibly could and we carried out the study and we received results that showed 50% reduction in cholera in the villages where they were filtering the water through sari cloth.
Well, this was very exciting because it allowed a very simple, inexpensive effective method for reducing cholera in developing countries.
It allowed us to provide a highly affordable technique for the villagers to be able to protect themselves against cholera. Now, it didn’t eliminate it, but we have some evidence that suggests that even of those cases that did occur, they were much milder.
Was this accepted in the villages by both the men and women?
The acceptance was nearly universal, 99%, so that we did not have to worry about whether men or women or children would drink water that was filtered. In fact, it became very clear to us that by educating the women, showing them water that had been filtered and water that had not been filtered, they could see in the water that had not been filtered things swimming, turbidity. The water that was filtered was clear. We could explain to them that this meant the water that was filtered was safer for their babies, for their children. That’s a very powerful stimulus.
Could you post a public health poster about this?
We provided a poster for the extension agents, the women who went village to village every two weeks, showing the kinds of things that are in the water-cocopods, plankton, zooplankton, phytoplankton, bacteria, etc.-and the women could actually see in the water held up to sunlight things swimming back and forth in the unfiltered water. And so it was very clear and very obvious, and I do think the adage is appropriate, “If you educate a woman, you educate a family. You educate a family, you educate a village.”
Isn’t it thrilling for you to know you had such an impact on this part of the world?
It is very exciting, especially when I got an e-mail recently from a colleague at Mott Lab where we did this study in Bangladesh that the cholera incidence in that area is at an all-time historic low. We are really, really very excited.
We are anticipating in the future studies being able to go a couple of steps further. What we were planning to do is provide the villagers with a very inexpensive bottle of hypochlorite solution-bleach-so that once the water is filtered, just a drop or so of hypochlorite chlorination will provide a level that will not be tasted but will knock out other microorganisms or any residual bacteria, and we think that this will be acceptable.
Right now if you chlorinate the water there’s so much organic matter that you have to chlorinate it so heavily that it tastes and smells offensive and so villagers will not drink the water that’s heavily chlorinated. But if we remove most of that, it will take much less, maybe a drop, of the hypochlorite solution, which would take us another step forward in providing a very low-tech method for preventing infectious diseases, other diseases as well as cholera so we’re very excited about this.
Now ultimately, in the future, we would hope that sewage treatment will be brought to the developing countries, but for the next ten or 20 years we need to have these kinds of low-tech solutions to a health problem.
What is the evolution of virulence, and does it play a role in infectious diseases?
It’s interesting: recent studies, one very recent study, showed something that we have really sort of known but it was elegantly demonstrated is that by passage through the intestine, there is an attachment of the bacteria to the surface of the intestine, followed by production of the toxin, and that those bacteria with the capacity to attach strongly and firmly become dominant in epidemics, and so you have a selective process for the more virulent form.
Now we have known, as microbiologists, for many, many years that if you wanted to enhance the virulence of a pathogen you just keep running it through susceptible animal populations in those studies, and that you could select ultimately for very highly virulent pathogens.
So when you have massive epidemics, you are in effect selecting for the most virulent form to be passed from person to person. So this is another component of the complexity at more or less the genetic level of an infectious disease but it’s tied into the population, so again we come back to this spiral biocomplexity from the molecular to the organismic to the community to the populations of the vectors, the populations of the hosts, the understanding of the environment and the interactions with the environment.
We suspect that those Vibrio cholerae with highly capable attachment mechanisms probably use these attachment mechanisms for some other survival mechanism in the environment and we’re exploring that now. But it all comes together in that viewing the human as simply marching through a forest or crossing streams of pathogens whose whole purpose is to infect us is not quite right. We are but one component amongst many biological components and we need to understand these interactions in order to better prepare ourselves, protect ourselves, to prevent the infection and the disease.
Do you think we can control the evolution of virulence?
There are many clever ways of controlling the evolution of virulence, particularly in diseases like malaria where the attachment and the passage through the malaria vector can be thwarted either by modifying the organism or by modifying the host and by providing, let’s say, a defective host.
Now this was done with insects in the southern United States by irradiating flies and releasing sterile male flies, and the populations were such that fertilization was ineffective, and you were able to curb the populations of the flies. Well, we can do this with mosquitoes perhaps.
There are ways of intervening, but again, you have to understand the complexity of the system in order to know where you can intervene effectively without having an immediate counter effect. Mother Nature is very clever and wily, and we must understand that it is more or less a chess game with Mother Nature that we must play.
What are the big unanswered questions?
We would like to export the technique for preventing cholera to other countries-Africa-where they have had some massive epidemics, some other countries of Asia. We would like to be able to work with public health workers to provide a global attack on the real diseases without eradication as being the goal. I think what we want to do is control and prevent, so that’s one very important factor.
What are the questions you need answered in order to be able to do that?
Well, we would like to know the role of the toxin of cholera in the environment. What is it really doing in the environment? I don’t think it is being produced by these bacteria simply to create disease in humans. I have a feeling that it plays a fundamental environmental role. Similarly, the attachment structures, we think that it’s part of a survival mechanism for the bacteria. If we better understand that, we can better understand how we can prevent the attachment to the surface of the lumen, of the intestine of humans. These are fundamental questions.
Also, we’re very curious about cholera as being a vector-borne disease. Now, people have never thought of cholera as a vector-borne disease, but you could think of the cocopod as a vector, and we might want to redefine vector-borne disease so that we would include some of these other diseases — Lyme disease, cholera, hanta virus, other diseases-as vector-borne diseases-you know a kind of broader definition of that.
In understanding infectious disease, we cannot just be examining the separate pieces of evidence more or less like reading tea leaves. We instead really have to understand the interactions, the complexity of the system, the global system, in order to be able to provide the public health for all peoples of all countries in the world.