



Rediscovering Biology: Molecular to Global Perspectives
HIV and AIDS Expert Interview Transcript: Jay Levy, M.D.
Professor of Medicine; Research Associate, Cancer Research Institute
Levy is a professor in the Department of Medicine and research associate at the Cancer Research Institute at UCSF. His research focuses on biologic, immunologic, and molecular studies of the AIDS virus, emphasizing viral and immunologic features of HIV pathogenesis and long-term survival. Dr. Levy’s group was one of the first to identify HIV, originally calling it the AIDS-associated retrovirus.
Interview Transcript
Levy is a professor in the Department of Medicine and research associate at the Cancer Research Institute at UCSF. His research focuses on biologic, immunologic, and molecular studies of the AIDS virus, emphasizing viral and immunologic features of HIV pathogenesis and long-term survival. Dr. Levy’s group was one of the first to identify HIV, originally calling it the AIDS-associated retrovirus.
What is a “nonspecific line of defense” in the immune system?
“Nonspecific” would mean a more generalized approach to an incoming organism that’s going to cause disease. It would be so generalized that you wouldn’t have to know exactly what that organism is; you just need to know something strange going on in the body.
If a tissue is damaged, what happens?
When the tissue is damaged, it can die by a variety of processes. The most common that we used to know about is when it just bursts and dies because it’s been hit or has had trauma. But there are other ways. It can secrete various proteins as it’s dying, and that will induce cells nearby to undergo what we call “program cell death,” or a term called “apoptosis.” That is a natural process. It says, “Things aren’t going well here and we want to get out of here,” and they die. That only increases the amount of cells that are affected by a trauma or an inflammatory something that occurs in the body.
So what are the most important elements-some of the basic elements if tissue becomes inflamed? What does the body do? What’s the first line of defense?
One of the reasons that we talk about inflammation is that it’s caused by part of the immune system. White cells come into a system where things don’t look right, and they try to remedy it. If they’re macrophages or what we call semi-dendritic cells-all partners in the immune system-they come in first. They eat up large molecules and then they grind them up, and they reflect what’s there on the surface of the cell. This then instructs other cells coming in what the nature of the pathogen-something that’s going to cause the disease-will be. Other [cells] will come in and won’t bother expressing what this pathogen is-they will just start tying to destroy it. And in doing that, they release certain substances [that are] toxic to that germ or microbe. Well, that will work, but it also affects the normal cells, and they will feel sick. So the basic idea behind disease is that most of the symptoms are due to our system trying to eliminate the organism.
You said they were releasing signals, or chemicals. What are those chemicals?
These proteins that are secreted by these cells have a variety of names. You can use a general term-“cytokine.” which is “cyto” for cell, and “kine” meaning attracted as a result of this encounter. Then you can have chemokines, interleukens, interferons, growth factors-a variety of smaller molecules. [These small molecules are] “natural innate factors”: [they] are really small, but they can go lyse a bacteria, for instance, and they could be defensens or protegrins. The general concept to remember is that these immune cells come in to fight off an organism. In doing it, they will secrete substances-a variety of them-to try to break open the organism or try to prevent it from growing and in doing that, they can create a toxic environment within the body. That’s what gives you your pain, that’s what gives you your headaches, that’s what gives you your coughs and your sneezes in a common cold.
Could you explain the difference between a chemokine and a cytokine?
Chemokines are part of the cytokine network. All of the substances I named are part of a cellular product, or a cytokine. The chemokines are produced by a variety of cells when they meet up with a microbe, and they live up to their name. “Chemo” means a chemical, “kine” means attracted, and they are releasing a chemical that will give out a signal to other cells passing by in the circulation: “Something’s going wrong here” and they come in. It’s very much like a pheromone in insects that attracts the female to the male, or the male to the female. We don’t know how it works. It’s fascinating. [Other cells] will see a very small amount of this chemokine-this is the white cell-and they’ll follow it until it gets stronger and stronger and stronger and then come to the point of the inflammation or the infection that’s taking place by the microbe. No one quite understands what the gradation is, and why they know to take that pathway.
Is that what the term, chemotaxis means?
Yes. Chemotaxis is part of the chemokine network-it may not be specifically a particular chemokine, but it will be the movement of the cells toward a chemical secreted product.
Now can you explain specific immunity? What’s the difference?
Specific immunity deals with a very precise targeted portion of a cancer cell, an abnormal cell, or a microbe. The nonspecific, which we call “innate,” picks up a pattern. So it could say, “It’s a bacteria, so I better react to it–it’s even a gram-positive or gram-negative bacteria. Sothey have something different on their surface and I will react to that. But I don’t need to know which specific bacteria it is” [Cells] could react to a virus-they’ll say, “This is a virus!” They don’t care what virus it is-it’s just not right. They’ll respond to it. That’s nonspecific. [The] specific, which comes later (because it’s the nonspecific that first responds), sort of goes in and says, “This is a herpes virus” or “this is the AIDS virus” or “this is the bacteria that gives you whooping cough.” So they are able then to discretely identify particular bacteria. Even further, they can actually pick out a small difference among the bacteria that are all part of a group.
How are they able to do that?
The specific immune system depends very much on the macrophage, or the phagocytic cell. Because it grinds up the microorganism into small little pieces-very, very small, maybe 8 or 9 amino acids. Then they get expressed on the surface of the cell. They then educate the specific immune system that comes in and says, “Oh, I see this particular small peptide-I’m going to respond to it.” They don’t know it’s herpes or HIV-they just see that. But it ends up that that is part of the nature of this microbe that’s now infecting the person. The specificity allows it to only hit that particular microbe and not take anything else that’s around, as in some cases with the nonspecific [response], which may get a person in trouble (although usually it doesn’t). So the specific can go right in, can get a large number of cells that are proliferating as a response to that education process
So the innate immune system really sets it up, then the specific can come in for the kill?
The innate immune system is often considered the first battalion going in. It’s the pawn in a chess set-it goes out, sees what’s going on. And then informs the specific immune system-the adaptive immune system-to respond. Now where does the adaptive immune system come from? That’s relatively new. All the tiny little organisms-insects and all the one-celled organisms that we have-they don’t have adaptive immune systems. They never developed it. We’re talking about an adaptive immune system that evolved a hundred million years ago. It’s said that this occurred when a primitive immune cell in the shark-when it developed a mandible-was infected by a tiny little virus, a transposon. And that created a total different immune cell, which can develop into specific subsets. There you get the B-cell that makes a certain antibody-all that’s directed by this type of process where you can get rearrangement of certain genes within the B-cell so it makes one antibody. [There are] rearrangements in the T-cell so that now it can incorporate a small portion of the microbe in a particular pocket, which has already been genetically determined by the rearrangements.
What’s the difference between humoral-mediated and cell-mediated immunity?
As part of the adaptive-or specific-immune system, we have cells that are called B-cells. They produce antibodies that are released by these cells and circulate in the blood, or throughout the body. Because they circulate and they aren’t attached to the cell, they’re called “humoral.” like humoral factors that are secreted. The cellular immune system has many more players-the macrophage, the dendritic cell that I mentioned before-they’re part of the cellular immune system. Then you have cells that are called “natural killer” cells. They’re part of the innate immune system, but they’re actually part of the cellular immune system, which permits them to go in and recognize virus infected cells or cancer cells and kill them. Then as you move up to larger populations, you get to CD-8 and CD-4 T-cells-or “thymus-derived lymphocytes.” These cells are a part of the cellular immune system. So you’ve got maybe 5 or 6 cells so far-there are many more. With humoral immunity, you really have the B-cell and the thousands of antibodies that they can make.
Please explain the difference between CD-4 and CD-8 cells.
When we talk about lymphocytes, we can separate them into the B-lymphocyte, that makes the antibodies, and the T-lymphocyte, that can then be separated into two different subsets, one that we call CD-4 and one we call CD-8. How do we get CD-4 and CD-8? They didn’t just arrive with the number, they were identified by particular reagents-which are monoclonal antibodies that are specifically made against a protein that’s on the surface of this particular cell. Because the antibody had a number 4, we now call them CD-4. “CD” is an immunologic term that is now used for all of the different subsets of white cells. So the 4 antibody went to the CD-4 cell, which is the helper lymphocyte. That’s the cell thatusually helps the immune system respond the best way. The CD-8 is identified by the number 8 antibody. And that cell has both the ability to kill virus-infected cells or cancer cells-or it has a function where it regulates the immune system. It suppresses an immune system that’s getting too active. Without the CD-8 lymphocyte, you’d have auto-immune disease [where] the immune system just goes chaotic and starts reacting-hyperactive. What is really coming through is a balance, which is a balance between humeral immunity and cellular immunity. We need both, but one may overpower the other and that’s not good for the body.
If you want examples, lupus, which is an auto-immune disease, has too much antibody; rheumatoid arthritis has too much cellular immunity. Why does this take place? We now know it all goes back to the CD-4 lymphocyte, which is the helper cell. Does that helper cell help humoral immunity? Or does it help cellular immunity? You have two types of helper cells: TH-1 and TH-2. So TH-1 CD-4 cells-T-helper cell 1-encourage cellular immunity. TH-2-T-helper cell 2-encourage antibody production. Then you might ask, “Ok, you’ve got those two separate CD-4 cells, they all have the CD-4 protein on their surface-what makes them different?” Now you get down to the understanding of the cytokines-what do they secrete? The TH-1 cell produces cytokines that help cellular immunity. Interleuken-2, interferon gamma. The TH-2 CD-4 cell makes cytokines that help B-cells develop antibodies IL-5, IL-10. Now they balance one another. So if the helper cells are really functioning correctly, each of them make just enough of their cytokine so the immune system’s functioning well. Otherwise, if they overproduce, they suppress the ability of the other helper cell to help that arm of the immune system. So what you’re seeing in the person whose immune system is functioning correctly, you have just the right amount of humoral immunity, and just the right amount of cellular immunity.
What is going wrong in a person with lupus? The T helper-cells that secrete protein that helps B-cells are overreacting. So the drugs you use attempt to target that reaction. Rheumatoid arthritis, multiple sclerosis-other diseases that we link to cellular immune abnormalities-have helper cells that are TH-1 type that are secreting proteins that are making that immune system too hyperactive. So the drugs try to target that particular T-helper cell.
To digress, when the immune cells come in and attack a foreign body, what happens to them? Do they die? Do they go back somewhere?
Very good point. A little more complicated. When a specific T-cell comes in and it attacks a microbe, or an infected cell or a cancer cell-and it creates a whole legion of cells that are going to do that-once they have destroyed a particular organism, there’s no more protein around, so they lose interest. Then what happens? They self-destruct. They go through what we were talking about earlier: program cell death or apoptosis. So you lose them. You’ll save a few of them-they’re memory cells-so if that organism comes in again, they can react very quickly.
Typically, what do antigens do?
Typically, when we talk about small pieces of an organism-or even a cancer cell that is recognized by the immune system-that’s called an antigen. So an antibody recognizes an antigen and the cellular immune system will recognize an antigen, realizing that this is all the adaptive-or the specific-immune system. Antigens don’t really come into play in the innate immune system. There, it’s patterns-they see a pattern of an organism. With the specific immune system-they pick up the smallest protein that will help them react against and organism. That’s an antigen.
Let’s switch gears a little to the HIV virus. Can you provide a real brief description of the virus-what it looks like?
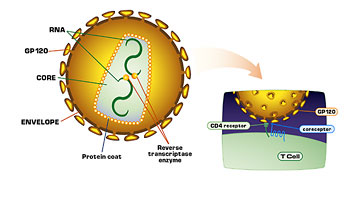
With the background of understanding what the immune system faces, it has quite a task of recognizing a variety of microbes. Not just bacteria and viruses, but amoeba and all sorts of unusual things that are not supposed to get in our body and cause disease. So along comes the AIDS virus. Have we faced a virus like that? We don’t know, but we suspect that if we did, it was-I think-thousands of years ago, and never really got going. What about other animal systems? Yes. These type of viruses have been around in animals for years-thousands of years. They’re called retro-viruses. Why are they called retro-viruses? Because when these viruses affect a cell, their genetic material is made out of RNA. Their aim is to get to the nucleus of the cell and be part of the chromosomes of the cell. What is the chromosome made out of? DNA.
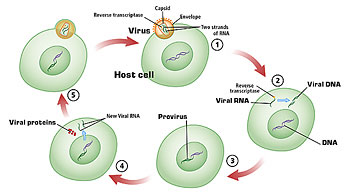
So these viruses have to find a way [to] like DNA, to get into the chromosome of the cell. They have an enzyme called reverse transcriptase, that was discovered about 30 years ago, which allows their RNA to make a DNA copy of itself. It exactly looks like RNA, but it’s a DNA copy. Then it goes-using that DNA copy-into the nucleus and it incorporates itself into the chromosome of the cell. It’s now like any other gene in the cell. This process of reversing-going from RNA to DNA-is just the opposite of what we call the genetic code.
Usually, the chromosome is what directs RNA to make proteins. Well, here was the dogma, until this enzyme was found and was recognized that these viruses have incorporated a way of becoming DNA, but the opposite. Backwards. They are made up of a lipid coat, fatty coat. What happens is when they meet up with the fatty surface of a cell, they fuse with that cell, and just the nucleus of the retrovirus goes into the cell. The centerpiece. Then the RNA comes out of the nucleus. Reverse transcriptase is attached to it and it starts making DNA. When it makes two copies of the DNA, like a chromosome, it goes into the nucleus and becomes part of the genes of the cell. Now, once it is in the nucleus, it can make the RNA and the protein and come out as a virus. Or it can stay latent, or silent.
That’s one of the most frustrating parts of trying to get rid of this virus: it can become secretive. It’s one of the few viruses that can do that. And thus, trying to get rid of it once it enters the body becomes really a daunting task-something that I think is virtually almost impossible. Unless the immune system can search out these silent cells and maybe induce them to make a little bit of virus, so they’re recognized, and then the immune system can take care of them. Otherwise, they can be there for years.
What is makes retroviruses different from other RNA viruses like influenza?
The fact that the retrovirus has an RNA puts it into a whole group of families of viruses that have RNA. Measles, mumps, influenza. [However], what is different about those viruses? Those viruses, when they enter a cell, have to kill the cell. Otherwise, that’s it. They can’t incorporate into the chromosome. So they are easier to control. Because, let’s say they kill a few cells. Then the immune system comes in, recognizes them and gets rid of them. HIV, the AIDS virus, goes in, the immune system recognizes it and may kill a little bit, but they’ve incorporated their genetic material in some cells and the immune system may not find it. Then they can pass that silently throughout the body, and you’ve got an established infection.
How does our own immune system help the virus stay there-help it to replicate?
If you’re looking at whether the immune system helps the AIDS virus or helps any of the viruses, the best way it does it is by trying to fight it and secreting these proteins that activate other cells to join the fight against the microbe. But what is the most susceptible cell to HIV? An activated lymphocyte. When these activated lymphocytes try to fight, the virus enters them. So it has more cells to infect. It takes advantage of the immune system.
Again, that’s one of the huge challenges faced in treating this disease, correct?
Yes, one of the questions that comes up then is: should you quiet down the immune system’s response against HIV, because then you’ll have a bunch of silent cells, but you won’t have this virus spreading throughout the body as it does when the immune system is so active. In fact, we know that people who have lived the longest with HIV infection, like some of our long-term survivors-their immune system is not as activated as people who are advancing to disease. With that activation comes program cell death, as we talked about earlier. These cells are activated, and after they’re activated, they self-destruct. New cells come in. Well, that self-destruction removes more important cells in the immune system, and you don’t have a defense against HIV.
Are you now describing the final progression? What happens at the very end stages?
Yes, so the question comes up-how does HIV cause AIDS? And the first answer must be: it doesn’t. What it does is allow AIDS to occur. Essentially, it presents the immune system with such an immuno-compromised state that opportunistic infections and cancers can develop. The definition of AIDS is not an HIV-induced disease, or an HIV-directly-induced disease. It is an immune-deficiency state that allows other microbial organisms to take over-cancers-and that’s the definition of AIDS.
Can you talk about the components of the innate immune system?
It’s important to realize that when you say “nonspecific” that’s not a pejorative term. These cells are the most important first components. They’re the ones that are going to see any microbes-they protect our skin from organisms from entering. They protect our mouths-all the mucosal surfaces. So now HIV comes in. It comes in as a free virus, and it can come in through infected cells. Infected cells in blood, or infected cells in genital fluid, in semen or cervical fluids. So it comes on to a surface.
It could be a surface in the vagina, or the anal canal, or in lymph nodes if it’s injected into the blood stream. The first line of defense-because you don’t have time for specific responses-is the innate immune system. It says, “This is something foreign.” And they enter. And how do they enter? They enter with components like macrophages-which play a roll in both types of immune system. And then there are components secreted by the liver and other cells in the body that float through the circulation, the blood, that can attach to HIV and kill it. You have what we call ‘lectins’, or binding substances that are attracted to sugars, like Mannose, so Mannose-binding lectins are part of the innate immune system. All of these are going to react very quickly.
Meanwhile, the message is going back. Why? Because when the innate cell is coming in contact with these micro-organisms, they’re activated. They start secreting substances. They secrete interferon, which is very powerful against HIV. But interferon also is a mediator of the immune system, and it activates the adaptive immune system. They will release chemokines-we talked about earlier-chemokines that are going to say, “We’re nonspecific, in that we’re just releasing these chemokines, but now let’s bring in all sorts of white cells because something’s going wrong in this part of the body.” So the innate immune system and its components-soluble factors, as I mentioned-like complement, and mano-binding-lectins-and cellular components. Like NK cells that don’t need to know that it’s a particular cancer cell, it’s just a cancer. It doesn’t have to know what type of virus is infecting, it’s a virus-infected cell. These kinds of cells come in and start working, they secrete substances that bring in the second legion. That second legion is now being educated. Because once the innate immune system recognizes this incoming organism, what are they doing?
Some of them are eating them up-phagocytosis. Then they express the proteins. Now they’re educated. So the innate immune system takes minutes to days to work. The adaptive immune system takes days to weeks. You need that innate immune system to give time for the adaptive to come in. The adaptive is generally so specific, it ends up being a very strong and massive attack on the organism.
So getting back to HIV then, why this is such an effective system-what are some examples of how HIV can be overcome?
We were talking about how HIV can infect the body through the blood, or through mucosal lining cells, and what happens-it comes in and the innate immune system tries to attack it and prevent it from infecting. But-in my opinion-the virus-infected cell is pretty immune, it lacks sensitivity, it can then come in contact with another uninfected cell and pass the virus right to the uninfected cell. Once it gets established in the uninfected cell-the cell of the individual being infected-unless the NK cell or some other cell is able to kill it within minutes to days, it can then spread. The innate immune system doesn’t do as good a job in curtailing that. Now it’s established and the adaptive immune system has to take care of it. How? They could make antibodies-neutralize the virus that’s being made, or they can make a cellular immune response, like CD-8 lymphocytes that are going to come in, and they’re going to kill the virus-infected cell. Something similar to what NK cells do, but very specific for this particular virus. It can’t be that successful because we only know of a few people who are able to get rid of the virus. These are what we call “highly-exposed uninfected people.” Otherwise the virus is there.
What happens then is the immune system controls the virus. It takes about ten years for the immune system to become so exhausted that you start getting symptoms of the HIV infection. A small percentage of people-5 to 7%-can go ten years or longer without any symptoms, and the virus is held in check, but it’s still there. These are what we call “long-term survivors.” Some of them are documented-we know, because we were studying their blood in 1978-that they’ve been infected for more than 24 years and are perfectly healthy. This is key because that’s the power of the immune system to control this virus. Something that was totally unexpected when we first found the virus.
But what you learn in virology, and in most diseases-there are always survivors. And you learn the most from studying them and that’s what we’ve done. We’ve spent fifteen years studying these long-term survivors. What we’ve been able to find out is that they have arms of the immune system that are working very well, and can continue to work to control HIV so it doesn’t give disease.
Before we get into that, can you comment on the fact that HIV is highly mutable? What happens?
One of the problems in trying to control HIV, and it’s true of many retroviruses in this group, is that when it replicates in a cell, it has a lot of mistakes. Most of those mistakes give rise to progeny, or what we call off-spring of that virus, which are dead. But there’s always some that survive. Mostly, those are going to be a little different than the virus that came in. So if they get more and more different, the immune system gets faked out, because it’s looking at the first virus. Now the third or fourth replicative cycle, they don’t recognize that virus, so they have to come in again. So obviously, we need a type of response that will take care of all these different subsets of viruses. Otherwise, the virus’ constant changing can cause an inability of the immune system to ever control it. This is one of the reasons why some people do succumb to AIDS and why it’s often said a vaccine will be difficult. I don’t agree with that, because I think we can elicit a response in the immune system-probably an innate immune response.
What happens to the viruses that survive?
I always think of viruses and microbes as obeying the same kind of laws that we have in nature-be fruitful and multiply. They’re just going to grow as much as they can to keep making more offspring. It has a Darwinian regulation as well, because “the survival of the fittest” is true. The virus that can come out more rapidly and infect more cells is going to be the one that’s selected. That means it’s going to have to go through some changes and it’s going to have to avoid the immune system. Some of the resistant viruses are going to be more powerful and will be harder to get rid of.
However, what we’re learning is that some of these resistant viruses are not as good. They can replicate, but they’re not as good. So one of the ideas is, maybe you force viruses to become resistant and they won’t be as powerful. That, I think, is a lot more difficult than finding an immune response that will take care of all these viruses.
I’ve read that some scientists are looking at ways to look at the viruses’ sloppy mutation as an advantage somehow.
Yes, that’s with drugs. [The goal is to] try to elicit a resistance to a drug in which the virus can grow in the presence of the drug, but the favored virus doesn’t replicate very well.
Can you provide a brief history of what HAART is and some of the problems that have developed?
Here we are with a virus that is able to replicate and spread, and we’re able to learn how it orchestrates its replicative cycle, and it uses three enzymes. It uses reverse transcriptase, which I talked about-which allows the RNA to become DNA; it uses “integrase.” which allows it to integrate or become part of the chromosome of the cell, and it uses an enzyme “protease,” which allows it to sort of cut the proteins into pieces, which are going to make up the structure of the virus progeny. When scientists learned that, they started to target drugs to those three proteins. Thus far, we have two of them that have been targeted successfully: reverse transcriptase and protease. So you have the reverse transcriptase inhibitors, the protease inhibitors and with time, we hope there will be integrase inhibitors. What happens is that they are able-in combination-to prevent the virus from mutating rapidly.
When we talk about “highly-active-retro-antiviral-therapy”-H-A-A-R-T-that’s when you put them together so they act the best they can. You’re targeting reverse transcriptase and proteases. Although now, we’ve even got to a point where you have three different approaches to hit reverse transcriptase, and maybe later you target protease inhibitors. But they’re all HAART therapy. It is very successful-lowers the viral content in the body dramatically until resistance develops.
What has happened with HAART with people who have been on it now for years?
HAART therapy became very well known in 1996. What we found was once you gave it to people who had AIDS, you completely reversedit. So the prevalence, the incidence of AIDS cases dropped precipitously. They continue to be reduced, but what is happening is individuals who are infected become resistant to these-there are now 15-drugs, and they do die. We aren’t preventing AIDS, we are delaying AIDS. And it’s extremely dramatic. We had a person see us who really had no hope in surviving, and he is now-from 1996 to 2002-on five different anti-retro-viral drugs. He’s doing extremely well. He’s back working, his immune system is back looking fairly normal. But he needs those drugs.
But what happens with some people who are on it long-term? What are some of the long-term effects that are starting to show up as chronic problems that these people are having?
We recognize that some individuals on these drugs become resistant to them so we have to keep changing them. But what was more disappointing was the fact that after these individuals were on them for a long time-one or two years-there’s a whole new group of diseases that develop. Because these drugs are not free of side-effects. What they had was disruptions in their control of fats. Their cholesterol went up. Their triglycerides went up. They started to get changes in their look. You had emaciated faces, very thin arms and legs, a big paunch called “Protease Inhibitor Paunch.” And a big hump in the back-buffalo hump-which you see with steroids, but you were seeing it with these drugs. You were getting diseases of the pancreas, diseases of the kidney, diseases in the liver. You were getting strokes. You got young people with heart attacks. So you couldn’t just casually say, “We’ll just put them on HAART therapy.” What you had to say was, “Let’s balance the side effects.” Something that I had advocated in 1996 was, “Let’s wait a while. Let’s not just give the drugs to everybody-let’s wait until they really need them.”
What you needed at that point was to appreciate that the immune system is very resilient. You can reduce the number of white cells to extremely low numbers. When you give HAART, in the majority of cases, they’ll come back. So if you can wait, you’ll avoid the side-effects. And that is now accepted clinical approach today.
So basically, this “really hit hard” approach that was touted a few years ago, is not being so generally used now?
Initially, the clinical physicians handling infectious diseases said, “We’ve got an infection, we’ve got to treat it. So you’ve got to treat it right away.” What they learned was, this is different from other infections. You can’t get rid of it anyway, and are you going to put these people on these drugs for their lifetime? These drugs in many ways resemble anti-cancer drugs. How many people that have cancer can stay on chemotherapy their whole life? We know they can’t-it’s too toxic. So they began to recognize that this wasn’t the approach. So today, the only time you would treat really early is in the first few weeks of the infection, where you really can try to block the ability of that virus to spread through the body. But after that, it doesn’t look like it’s worth treating early, but wait until the subject needs the drugs.
Would you have to catch the person right after transmission for this to be effective?
Our laboratory’s involved now in a study of what we call acute or primary infection. [These are] individuals who have the symptoms of acute infection-which looks like the flu-but you find that they have virus in their blood. They may or may not have antibodies yet-then you can put them on drugs. Most studies thus far say it probably helps, but we need years to know if it helps. All you know is yes, you reduce the symptoms, you reduce the virus. Their immune system looks better. But what’s the long-term effect? We don’t know. Even better is someone who comes in and says, “I think I’m infected-the condom broke.” Or, “I used an un-sterile needle and I think I injected myself with HIV,” and you then check, and if you find the virus is there, there won’t be any immune system response. You give them drugs-that may be even better, because there you could probably curtail the virus, and prevent it from really spreading and doing any damage in the early stages.
So given all this, why do you feel the emphasis should be on the innate immune system?
First, let’s say we certainly have appreciated what drugs can do, and when they are used at the right time, they are really, quite miraculous. But we also have to recognize that long-term survivors have told us: You don’t need the drugs. The immune system has the capacity to control this virus. What did we learn from the long-term survivors? We learned that there are components to the immune system that are functioning. What we would like to do is bring that knowledge to everybody who is infected and try to stay away from these toxic drugs. However, [we’d] use drugs or compounds that are going to boost the immune system and bring the control of the infection back to the individual who’s infected.
So you’re trying to find one of the secretions that you were talking about earlier that’s coming from CD-8 cells? What is CAF?
In our studies of long-term survivors, the one feature of their immune system that constantly came up was a function of the CD-8 lymphocyte. That’s the adaptive immune cell that usually kills the infected cell. But what we found was that this cell in HIV infection doesn’t necessarily kill the infected cell-it secretes a protein which we call CD-8 antiviral factor, or C-A-F, that suppresses the virus in the infected cell so it cannot produce anything. That cell is carrying a silent gene and can function. We think it works quite well, because it brings function back to the infected cells. Gradually, those cells are going to die with the virus. But what happens to the long-survivors is they have a strong CD-8-what we call non-killing-anti-viral response and that virus is there in extremely low amounts. If it happens to get produced, the cells come in and suppress it again. What we are doing now is looking at what the protein is that they make. Because it is active against all HIV strains, active against the monkey AIDS virus, it’s nonspecific. So therefore, it has to be an innate response. It fits that it’s an innate response, because it’s mediated by a secreted product.
In general, most secreted products of the immune system are innate. They’ve been around for years. We are trying to bring back that innate immune response to people who are infected. What you’re really saying is allow CAF production to return and now you’ve brought control back to the host.
It’s not produced in a large amount, but it’s really potent-is that true?
What we know is-like many of the secreted products of the immune system-they aren’t meant to be made in huge amounts because in cells they could be toxic-they could activate cells. They’re meant to be produced when the CD-8 lymphocyte meets up with an infected cell. So over that short channel it’s produced, it is very potent. Now you go to try to identify CAF, you take those CD-8 cells and put them in a culture dish with growth media, and you’re asking it to produce CAF. What you find is that the CD-8 cells are making many other products that make the identification of CAF extremely difficult. We will get there, but that’s the problem. What we will try to do and what we’ve been learning is, “How can we get the CD-8 cell to return to making CAF?”
I’ve read that there’s only about 1% of the population that are non-progressors, so you don’t have a large population of people to draw upon to study. Is this another problem?
No. What we know is that most people, when they’re initially infected, elicit this response, right? It’s an innate response. But over time, they lose it. The people who maintain it are the long-term survivors. Or the long-term non-progressors. We can study people while they’re healthy and look for this factor. Now what we learned recently is the product interleuken-2 (which is made by the CD-4 lymphocyte that’s part of the TH-1 responders, which help cellular immunity) when given to CD-8 cells that have lost the ability to make CAF, start making it. It’s why we’re encouraged by some the trials that are being conducted, giving interleuken-2 to people with therapy to boost the immunesystem, which we think boosts the CD-8 response. Unfortunately, interleuken-2 can be toxic itself, so it’s tough for people to keep on the drug. They pulse it-in the studies that we know of-every two months, and we’re doing some of that. Also, we know that the CD-8 cell, when it comes in contact with the macrophage-or more specifically, the dendritic cell-gets signals which restores its strength. So if we’re able in the library, to get dendritic cells and put them in the culture dish, put in CD-8s that have lost their activity, leave them for three or four days, and take them out, they’re able to restore the function. We know that’s mediated by another cellular product.
This sounds like a terribly painstaking process. You’re trying to narrow down to a very specific gene and protein, correct? How do you analyze just one gene at a time?
Where are we with finding this cellular factor? In the early days, which means ten years ago, we were trying to figure out if it was something we knew. We had to rule out something like thirty different cellular products, including the interferons, the chemokines, and the growth factors. That took us a long time. Then once we realized it’s novel, we asked, “How are we going to find it?” It’s one in a million proteins produced by CD-8 lymphocytes. So now [we’re using] modern technology to find a protein. That’s really interesting because we couldn’t have done it ten years ago.
What are we doing? There are certain ways of purifying the protein now, using proteomics, that weren’t available three or four years ago. We’re using that approach- so we have this fluid-and we’re getting rid of all these proteins that are not CAF. Then we get down to where we think CAF is, and we give it to a laboratory that does what we call “mass spectrometry.” They put a beam of electrons in and break up the protein and that computer tells you what the protein is-in the old days it could only pick one protein out of a group. Now it can pick up to 20. So we’ve really helped! That’s one approach.
The other approach we do-along the lines of finding the gene-is to take the approach of microarray technology. A microarray chip is a tiny little slide that you can now make with every human gene spotted-that’s thirty-six, thirty-eight thousand genes. Then you take the genetic material from the cells that are making CAF and the cells that aren’t making CAF and you put them on these slides and ask, “What is the ability for this genetic material to attach?” It attaches to a gene that it recognizes. What you find is, the CAF-positive cells will bind to certain genes that the CAF-negative will not. There may be a lot of reasons why not, so you then have to narrow it down. We’ve had three approaches, we started out with two thousand different genes, and then down to five hundred and down to two hundred, and now we’re down to forty-four.
We hope that we have one of the genes. One of the difficulties in the molecular approach is that along the way you can’t constantly look to see, “Is this an antiviral protein?” You’re just looking at a gene. Whereas with the mass spectrometry, you know all along the line, “It’s still suppressing the virus.” With the molecular technique, you take two years, you end up with these genes, and then you have to take those genes, put them into a cell, and have the cell make the protein. And you hope one of those genes is CAF.
And then do you have to go on to prove that it will actually have an effect against HIV? Do you have to do another step after that?
So after you found it’s CAF, then the approach will be to determine if you can you give CAF to people, or should you find a way in which you can tickle the CD-8 cell so it makes its own CAF? Which is the one I would expect. Frankly, once we find CAF, there will be so many people jumping in that it won’t be very long before this will be a major way of treating this disease.
And, you said you can either synthesize it and make a drug-or let the body stimulate it. You can put it into vats and make lots and lots of CAF protein, purify it and give it to people. You can cut it into small pieces and only find that piece which is the most active and give it as a small molecule-that’s good because then you probably could eat it-take it as an oral medication-otherwise you’d probably have to inject it. Or you could find small compounds, that when you treat CD-8 cells, they suddenly make it. That would be terrific. These are the approaches that will come about once we’ve identified CAF.
There is a dispute, isn’t there, about whether or not this is one gene ore more than one gene responsible for making CAF?
Yes. Does CAF have to be one protein? It doesn’t. But many of the procedures we use to identify CAF involve heating and changes in pH and it’s still there. It just seems to me that you’ve got one major protein. There may be another. There are groups who are finding all sorts of anti-viral proteins. Which is gratifying because this is a field that was never explored before. A secreted anti-viral substance that’s not interferon that’s working against HIV? No one gave it any attention. And then someone realized-I think that most scientists are realizing-there’s something here. So then they start looking. They use all sorts of assays, they use all sorts of cells, and they’re coming up with new products, and already-known substances like chemokines, and saying, “They work against HIV.” Terrific! Make a drug from it. But what are we interested in? What’s the secret to long-term survival? It’s not production of chemokines. It’s not production of some of the other proteins that have been discovered. There is no clinical relevance. They may be antiviral, but what is the secret to long-term survival? It’s CAF. And CAF is not any of those products.
So while there are five or six groups now going after CAF, along the way they say, “We found it-it’s this. We found it-it’s that.” The key questions to ask: “Is it produced by normal CD-8 cells in response to HIV? Is it found in long-term survivors and not in people who advance to AIDS? Is it a common finding in people who can control the virus?” These are just some of the questions you should ask. All these things we went through in the very early days to prove to our scientific colleagues that this is an immunologic response that is important. Originally because it didn’t kill the infected cell, yet it was mediated by a CD-8 lymphocyte, they said this can’t be important. You can see now why the emphasis in today’s science on the innate immunity is helping a lot. Because we believe this is an innate immune response.
So the common denominator for long-term survival, is it just CAF? Is that the bottom line?
There are many groups that are trying to figure out why these long-term survivors are doing so well. We found the CD-8 non-killing-type-response, which we think is a very common denominator. Others have found that the virus may be weak-it lacks some good genes. But when we’ve looked at people that have those types of viruses, what is the common link? CD-8 antiviral response. So if you have a weak virus, the immune system can control it. Then there are people who lack-on their surface-a receptor to bind to HIV, called CCR5. Well, it’s only one group of viruses. There’s another group of viruses that could get in anyway. What have we found? We studied some of those. They do not have the virus, but they have the CD-8 antiviral response. I think they met up with it, there was an innate response, kept it away-the fact the virus couldn’t get into the cells as easily as others allowed a good control.
So my conclusion is, if this is-if not the most common finding-it is certainly equally important to almost anything else we’ve seen, and I do believe it is something that we need to induce with the vaccine, and we need to find a way of inducing it in people who are already infected so that they can control the virus.
You were talking about non-progressors and slow progressors. Could the non-progressors just be really really slow progressors and maybe go on and develop AIDS at some point?
Often people ask, “Will your long-term survivors or long-term non-progressors progress to disease?” The quick answer is, “Some of them have.” But there are those-like some people who are affected for more than 24 years-who would say to us they could control it. One of the reasons I named these groups “long-term survivors” and not “non-progressors,” is because non-progressors sounds like eventually they will progress. I like to call them long-term survivors because I think they will be long-term survivors. I’m not naive to say that none of them will progress, and some do, after 15, 18 years. But it becomes less and less likely as they get further out. It looks like they really have caught on to something.
Was Erik von Muller one of the first long-term survivors that you worked with? Did he volunteer very early on this, or how did you become associated with him?
Erik was among the first that we started studying in the mid-1980’s. He was one of the models for long-term survivors, but in those days, long-term survival was two years, three years. So now you’re twenty years and he still continues to do very well, he controls the virus, has good CD-8 responses, so he’s a good model.
When you first met Erik, did a light bulb go off when you started working with him?
Our first recognition that some people were going to control the virus didn’t come from Erik, it came from some people we saw earlier. We saw Erik maybe ’86 or ’87 and we discovered this in ’85, reported it in 1986. A group of people whom I had been following who had come in ’83, when we were first getting the virus. We thought that we couldn’t get virus out of these people, and yet they were infected because they had antibodies to the virus. That’s when we thought that maybe there’s an immune response. Since the CD-8 cells are the most common anti-viral cell, we took the CD-8 cells out of the blood sample that we had, by certain techniques-and the virus came back. It was very dramatic. Then we put the CD-8s back, and the virus went away. That was the big surprise. Then we started to say we wanted to talk to other people.
As people came through, we would ask: “Can they remove the virus easily? Or do we have to remove CD-8 cells to get the virus?” And that’s when Erik came. We found that unless we removed CD-8 cells from his blood sample, we couldn’t find the virus.
These long-term survivors are providing a wealth of information for you, but the bottom line is hope for other people with HIV. Are these type of people offering hope to you and those that are infected?
When I was trained in virology, I was told by my mentors-particularly Warner and Brigitta Henley who discovered Epstein-Barr virus in infectious mono-they said, “Jay, you’re going to learn the most from people who survive infections.” And mostly, that’s 99% of people. But in HIV, it’s only 5%. It didn’t matter. These people represent our closest eye into how nature can control HIV. And if we do nothing, then by simple genetics, they will be the survivors of this massive epidemic. We want to find out what’s different about them-what’s the secret? They are wonderful contributors. They come every month to my laboratory.
Not to say they aren’t going through certain feelings themselves because they feel so fortunate and they feel sorry for those that aren’t in their position. [There is] this sort of survivor’s guilt. They recognize that their contribution to finding the final solution is going to be their reason for doing so well.
For someone who’s infected with HIV-can you rescue the immune system and turn them into long-term survivors? Can you reverse the process?
Our big hope would be that you could take someone whose immune system is crashing and bring it back so we could control HIV. We mentioned interleuken-2. That may be one way in which you could do it and I think that it will begin to work. There are other natural products that seem to work. Interferon itself helps. There’s a product called interleuken-15 that may help. So bring them all together. What is the problem? The problem is, there isn’t enough resources. There aren’t any companies-major companies-who are looking at the immune system to boost it against HIV. They want the very quick fix. They want to target the virus and get all the drugs against the virus so every drug is against the virus.
There’s no therapy-except interleukin-2, now-that’s boosting the immune system. We really wish there would be more of an emphasis on the immune system. After all, that’s what we’ve been discussing today. If one could enlist and harness the immune system, it’s a more natural way, and we’re learning from these long-term survivors how important it can be.
Can you briefly give a global perspective on the problem of HIV and AIDS and the need to continue research? How are we going to help these people now where it’s just devastating countries and economies?
Of course, the big question now is-and it’s vying groups against one another-do you encourage prevention or do you encourage treatment? There is no question that now that the world knows that there are drugs that can help people who advance to disease, we cannot deny them the drugs. There is evidence to suggest that if you give drugs to people, itlowers the amount of virus in their blood, and also in genital fluids, so you may actually reduce transmission. This doesn’t mean that if you’re on drugs you can go and not worry about transmitting it, but there is some evidence to suggest that.
So we’ve got to do something worldwide, and it’s being recognized. You can’t look at the world and see what’s happening with 15,000 new infections every day and 8,000 deaths every day-and just sit back and be oblivious and not respond. What we need is cheap drugs, and that’s coming about through processes-companies in Brazil, companies in India, China is now mounting some companies to produce the drugs. They’re able to get it down to a $1.50-$1.10 a day for some of these therapies. That’s very good, except that you’re talking about countries where ten dollars a month is a good salary. But you’re seeing that.
What do we hope? We hope that when we find CAF that it’s going to be really cheap to induce it to be made. Then people can take it by mouth, and that’s going to give control to everybody. There won’t be any toxicities because you give these drugs to people, you need to have physicians to monitor them to see if they get sick. You don’t want low levels of the drugs to be present in the bloodstream so that resistance to the drug can occur. So all these problems are there. They’re often talked about as the reason why we have difficulty giving the drugs out. But they cannot hold any merit now. We have to get the drugs out. We have to train the physicians to give them-that’s going on-and we have to help all the people of the world.
How do you train the physicians when you’re talking about a lab that maybe has a couple test tubes? How do you even fathom helping these people with the infrastructure they have and the lack of supplies?
There’s no question that we need a whole new concept and approach for bringing antiviral drugs and treatment to many countries in the world. But it will take place. Some countries-their infrastructures for public health is extremely well-developed-like China. Other countries, not so. We won’t be able to do it tomorrow. I think that’s the message: “Don’t expect it overnight.” First, define the problems. The problems are to get cheap drugs. And find a way of giving it. And finding people who are trainedsufficiently. They don’t have to be trained doctors. They can be nurses, or nurses’ assistants. They can see these people, monitor them-if there are any toxic effects, find a way of treating them. It is approachable.
But I want to emphasize that we should not lose sight of prevention. What’s happening is all the funds are going for treatment, and we’re saying, “Fine, we just treat, that’s it.” We aren’t looking at blocking this epidemic. I’m not sure how it can be done, but we must not lose sight of the fact that we need to prevent it through education, distribution of condoms, needle exchanges, and of course a vaccine. A vaccine is the whole new topic, but what you need to do in a vaccine-as a final word-is you’ve got to block the free virus and the virus-infected cell. That is something we’ve never had to approach through a vaccine. We’ll do it, because I’m optimistic about that, but it’s going to take some creative thinking.