




Rediscovering Biology: Molecular to Global Perspectives
Emerging Infectious Diseases Expert Interview Transcript: Lukas K. Tamm, Ph.D.
 Professor of Biophysics, University of Virginia
Professor of Biophysics, University of Virginia
Tamm is a professor of Biophysics at the University of Virginia where he is studying the structures and interactions of viral fusion proteins in lipid bilayers, mainly using the influenza surface protein, hemagglutinin (HA). This research opens possibilities to develop new classes of viral entry inhibitors, which would serve to prevent influenza infection.
Interview Transcript
Tamm is a professor of Biophysics at the University of Virginia where he is studying the structures and interactions of viral fusion proteins in lipid bilayers, mainly using the influenza surface protein, hemagglutinin (HA). This research opens possibilities to develop new classes of viral entry inhibitors, which would serve to prevent influenza infection.
Could you comment a little bit on the 1918 influenza epidemic and how devastating it was?
In 1918 there was a so-called Spanish flu pandemic and suddenly many people died, about 20 to 40 million worldwide. I think it’s believed that American soldiers in WWI actually brought it over to Europe and it became a large pandemic in Europe and from there it spread all over the world. I’ve even heard that some historians claim that maybe the Germans lost WWI because they lost so many soldiers to that Spanish flu in 1918, or at least that was a contributing factor to it.
So what is it about the influenza virus, how can it do so much damage?
It is very infectious, as everybody whoever got the flu knows, and most of us have had it. But with most flu infections, they are not deadly. Usually, you can overcome this. Your immune system fights it and eventually, you get healthy again. Some of these viruses or strains of viruses appear to be particularly vicious and claim more and more or claim very large numbers of death. And it’s actually not so well understood, even today, what causes a particular strain to suddenly set off and be so vicious and so virulent compared to the others that are circulating the population all the time. So as we just said, in 1918 there was this large Spanish flu as there were many in previous centuries. That was over a particular strain that we call H1 N1. And then, I believe, in 1957 or around there, there was an Asian invasion of new strains they are called H2 N2. And actually the H and N stand for the major surface glycoproteins. So they have variance in those. First, in the Spanish flu they were the number one variance and the Asian flu pandemic in 1957 it was number 2’s. Then in 1968 or the next one and that was the last major pandemic and that is an H3 strain for H for hemagglutinin which is the major surface glycoprotein of these viruses. And that came from Hong Kong. So we call these the Hong Kong strains.
Is it cyclical? Is it every 20, 30 years that some of these really virulent strains take hold?
As far as I know, it’s still not very well understood and it’s still more or less erratic. The Center for Disease Control, for example in Atlanta, and many other national health organizations monitor that very closely, year by year. And try to figure out where to prevent a serious pandemic from happening again, or to catch them very early. There was an incident in 1997 where a new strain called the H5 strain appeared in Hong Kong again. That was transmitted from birds, actually chickens to humans. It appeared to be a very virulent strain so all the health organizations were very concerned that this might be the beginning of a new pandemic but they could catch it very early. They actually sacrificed the whole chicken population in Hong Kong in that year. That may have contributed to suppressing that pandemic. I think it was later also found out that this particular strain was not as infectious when it jumped from human to human so it was very infectious going from chicken to man but not between humans.
What kind of virus is influenza? What is it composed of? What does it look like?
It belongs to the class of so-called enveloped viruses and that means it has a membrane around it. Some other viruses don’t have that, they have a so-called nucleocapsid, which is a protein shell with the RNA or DNA inside that. In the case of these enveloped viruses. They have a lipid bi-layer membrane around them like our cell membranes, very similar construction. Then they have 8 RNA segments. Influenza has 8 RNA segments inside that bag or vesicle. That vesicle is about 100 nanometers in diameter. That’s ten to the minus 7 meters. So a tenth of a million of a meter in diameter.
What could you compare those 8 segments of RNA to?
So they are like the genes or they contain the genes of the virus and they could be compared to the chromosomes in an animal cell. Only that they are much smaller and that 6 of these 8 segments code for just one protein each. Two of those segments contain code for 2 proteins each. So the virus actually makes 10 of its own proteins. And the genes are located on these 8 segments.
Ok and tell me when you look at the virus, what is it surrounded by? What does it look like?
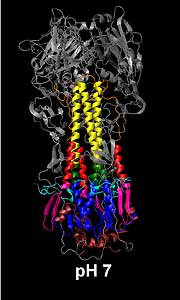
Right. So let’s go from the inside towards the outside. So from these 8 segments if you go outside you find first a layer of protein called M1 and on top of that you find this membrane envelope that I mentioned already. And inserted into that membrane are three different types of proteins. The two most abundant ones are the HA, standing for hemagglutinin and neuraminidase. Both of the proteins project long spikes from the virus surface and that can be seen very well in an electromicrographs of these viruses. The amino acid, spatial, three-dimensional structure of those proteins have been done, the structures have been determined for both the hemagglutinin and the neuraminidase. Actually, on the other screen, the structure of both of those structures are structures of the hemagglutinin in two different shapes, or two different forms. One at neutral ph, that’s in the resting form how it would sit on the surface of the virus. Then a low ph form which is important for the infection.
That’s what you think. That’s a depiction so you don’t know for sure? But that is pretty much from what the data tells you it would look like if you could actually look at this thing right?
Right exactly, so yes we are sure that it exactly looks like that. I mean the x-rays really gave a detailed picture of it. It’s not a microscopic technique where you could see it directly with your own eyes. You get sort of indirect data that are very in precise and then you can build your structure back from by computation from those data. This is exactly what it looks like so it’s not just only a model or an imagination.
That’s something, that’s brand new stuff. Could you do that 5 years ago?
Well actually, the crystal structures that you see have been done by Don Wiley’s lab at Harvard and the structure of PH7 actually was done 20 years ago. And that was big, big news back then. Then the other structure, the PH5 structure came about in 1995 I believe or 94 from the same lab. Our lab is more interested now in how these structures fit into membranes. What are these structural changes that occur from the PH7 to the PH5 form. How do they couple into membranes and Actually poke a hole, so to speak, into the cell. To let the virus in. So that is one of the major functions of influenza.
What are some of the challenges in trying to control this virus. What makes this virus unique?
Well one of the challenges is, of course, that is has a lot of antigenic variability, so each winter when the flu comes around again the composition of those HA an NA molecules or sub variance of it will be different. That’s why we need a different cocktail of flu shots every winter.
So a genetic makeup of the virus is actually mutating and it mutates every year? How often do these changes happen?
Well, it can potentially mutate by anytime by any passage. You have to imagine that these viruses in any single body make probably millions of copies of themselves in a single person each time. So every time it replicates it’s RNA and makes more copies of that there is a certain error rate and they could make some new mutants. If these mutants happen to be on the cell surface in the hemagglutinin or in the neuraminidase then they may escape immune surveillance in our body. So they would elicit a different set of antibodies there that we may not have at that time.
Tell me why does the virus mutate? Maybe define re-assortment and antigenic drift and what ramifications that has for our body to fight it.
Right, so I think the reassortment is actually the reassortment of these gene segments or RNA segments that we talked about. That happens more on a decade time scale. So it is a relatively varied event and that’s when these new pandemics happen. But the yearly changes we see in the population when we need new vaccines every year are sort of secondary, minor changes, that happen in the antigenic determinants on these surface, glycoproteins. On the hemagglutinin and the neuraminidase.
What happens then? They just mutate?
So they just mutate spontaneously as you go, whenever these viruses multiply in an individual’s body or are transferred to a new human. Each time they replicate they have a chance to make a reading mistake and make a new mutant. and if that mutant can survive it can take the majority in the strain and eventually will take over if you don’t have antibodies in your circulation to fight it. So a new strain or a sort of new sub-variant can then become the dominant virus in your body or in the population.
Can you define the difference between a pandemic and an
epidemic?
Again I think a pandemic is very similar to an epidemic except that the pandemic is sort of much larger in magnitude. In pandemics, there is mostly a major re-assortment of these RNA segments happening. Whereas in the epidemic may be pretty large changes, but not as dramatic ones happen in the pandemics.
Is epidemic more regional or local? Where pandemic is more global?
Probably yes. Probably yes. I think you know that is still active research not in our lab work. But sort of more epidemiologically orientated labs where they really want to figure out what triggers a new epidemic, or particularly a pandemic. So one still does not understand that in full detail.
What are the natural reservoirs for the subtypes of influenza?
There are, if we classify say by the influenza hemagglutinin, for example, there are I believe 13 subtypes, maybe 14. We have talked mostly so far about H1, H2, and H3 which are the first three, and they are the major ones that occur in humans. But many of these other subtypes occur in other animals. Some in pigs, in swine. Some in horses, there is a horse flu. All of them actually occur in birds. In a variety of birds. Chickens, ducks and so on. So the birds are actually the largest reservoir of these different subtypes of flu. Man has some of these subtypes like H4 and the higher H’s have never crossed into humans.
If they carry this virus with them all the time why aren’t the birds getting sick?
It’s more in the intestine for birds, they don’t sneeze of course so they harbor it more in their intestinal tract as far as I know and they secrete it and transfer it from bird to bird also that way actually. So it’s very different symptoms from influenza in humans, it’s the same virus or group of virus, but it has very different symptoms in birds or in horses.
You mentioned that not all types of bird viruses can infect humans though right, or do you know?
Not all bird viruses can infect humans. So there was an incident, we talked about this briefly already, in 1997 where this H5 subtype which was only thought to occur in birds and was known to be in ducks and chickens before, then suddenly infected some humans in Hong Kong and that triggered this large scientific activity and the health maintenance activity to try to contain that. Because people were very afraid that it might trigger a new pandemic.
So does there have to be some sort of intermediate host for some of these viruses to jump from birds to humans?
Yes, so I think you know at least before 97 it was commonly believed that pigs have to be intermediates, so it goes from birds to pigs and then to humans. And but I think in 97 those H5 incidents it was shown that these H5 viruses could jump directly from birds to humans. So that sort of changed the paradigm.
We were talking about pigs. Do birds’ viruses reassort in pigs to a point where then they are in a point where they can infect humans? Is that how they jump from chickens to pigs to humans?
So they can infect humans often because they go from birds into pigs and then from pigs into humans and they often during that process re-assort their genes and get a more virulent combination of genes that maybe have more virulent HA’s or NA’s on them. So that’s how we get infected with new strains.
How are we getting infected with the virus? How does it jump from pigs to humans?
I am not exactly sure but I think you know it’s probably workers that handle pigs. I think at least with birds it’s believed that the bird is contaminated on the surface and then somebody on the market handles it and doesn’t wash their hands, and so on, and that’s how it happens and I could imagine that similar things happen with pigs or pig handlers.
What are HA and NA?
So hemagglutinin (HA) and neuraminidase (NA) are spike glycoproteins that protrude from the virus surface by about 10 to 14 nanometers. So these proteins are quite large proteins. They have different surface loops. The protein is, of course, folded up as a chain of amino acids. So some of these amino acids would be located on the surface of the protein, directly accessible to the environment. Those amino acid residues would be the most that would constitute usually antigenic epitopes. Those that are seen by the environment and that could be accessed by antibodies in our body.
What is hemagglutinin’s role? Why is it there? Talk to me about how this helps it attach.
Right so hemagglutinin has two different functions, both packaged into the same protein. The first function is to attach it to the cell surface, it does that by attaching to particular sugar residues that are always present on all animal cells. So that’s why influenza can infect in principle so many types of cells because its receptors are very abundant and very ubiquitous on cell surfaces. So that is the first function. Then the second function is a so-called membrane fusion function. After attachment to the cell surface, the influenza particle gets internalized into the cell, engulfed into what is called an endosome. A so-called endocytosis. So it ends up in this little endosome and the PH in that endosome is lower than in the environment. So neutral PH is PH7 and so the PH typically in those endosomes is PH5 so that’s a higher proton concentration. And that PH change then causes this hemagglutinin to change it’s shape very dramatically. That in turn, that shape change when it is connected or linked between the virus and the cell or the endosome membrane, that big shape change then opens up the endosome membrane and lets the virus in.
Tell me then how is this different from the HIV virus?
So the HIV virus is also an enveloped virus. So in that sense it belongs to the same structural class. It is also an RNA virus. Although it is genetics work very differently from influenza genetics. But it enters the cells also by receptor attachment first and then by membrane fusion. But in contrast to the influenza virus it does not have to go through this intermediate step of the endosome at the low PH step. So it fuses directly at the cell surface. It binds to its receptor, which happens to be in HIV on the lymphocytes, and then the trigger for the shape change in that molecule is then receptor binding, and then it does the same thing, it uses a very similar mechanism to hemagglutinin to actually change its shape and poke the hole into the cell membrane directly at the surface and let the HIV particle in.
But the HIV doesn’t use the sugar, its receptors are different?
Exactly, the HIV uses the so-called CD4 molecules and the coreceptor that are specifically found in only a few cell types, like lymphocytes.
Are these two or three molecules, playing a vital role if the virus is resistant to a drug or becomes resistant to a drug? Is it these changes in these molecules that are mutating the virus?
Well we have to distinguish between antigenic resistant switches or antigenic drift. When these molecules change their surface loops, as I explained before, they sort of evade the immune system. So a flu shot is not really a drug. That is, you are administered that virus and that makes antibodies, so that is the natural immune defense of ourselves. But there are also drugs that are used in severe cases, or especially for elderly people, to prevent the flu virus from growing and two of the drugs or some of the drugs that are known inhibit a third membrane protein that we didn’t talk about much so far. This is this little M2 protein, which is a channel protein. It makes a little hole in the virus membrane itself and lets protons in when the PH changes, the endosome. These protons will diffuse through that little pore into the virus and that let it do all this conformational change of the HA that we talked about before. So these drugs block that proton channel. And so in that way the virus can be stopped. And the second class of drugs affects the activity, or inhibits the activity, of the neuraminidase. So, these are so-called neuraminidase inhibitors. They first were channel blockers.
What does the neuraminidase molecule do?
The neuraminidase molecule represents about 15 or 20% of these glycoproteins on the surface. And it has a similar size. It’s also very large, similar to the hemagglutinin. It’s function, it is an enzyme. So it can cut these certain sugar residues off of proteins that are in the neighborhood. That would be put onto the hemagglutinin in its biogenesis, when the fresh hemagglutinin is made in the cell for the progeny virus, it goes through a stage where it would have its own receptor packaged onto it. So the neuraminidase has to trim those sugars off the hemagglutinin so that virus does not try to infect itself or bind to itself. So that’s what the neuraminidase is important for.
How does the virus get out once it gets into a cell? How is it able to detach and infect new cells?
So that’s actually almost a rebirth process of what we talked about with the infection. So, it’s a membrane budding process. So what happens is the viral RNA’s code for these 10 virus proteins, they are made in the cell. Three of them we said are membrane proteins so they get inserted into the cell surface membrane and dissemble there in little patches. And all the other proteins and the newly made 8 RNA segments find that little patch on the cell surface and then it pinches off in a budding process and it makes new virus particles that way, multiple times. So many, or hundreds probably, of new virus particles could come out of a single cell that way.
So the HA and the NA don’t have anything to do with the budding phase and it leaving?
That is still not so well understood, how those membranes are actually constricted off. These HA certainly, and NA also, are known to assemble into discreet locations of the membrane surface. They have signals to do so encoded in them. So sometimes these are called lipid rafts, they contain a sort of cholesterol which domains in the membrane, that is where these proteins go to. That’s where new virus particles are formed.
Let’s talk a little bit about the ramifications of your research. How is it going to translate into public health strategies maybe or better drugs? How is this going to help?
Obviously all of these drugs that we already Mentioned, like the channel blockers or especially these neuraminidase inhibitors, were drugs designed after the structures of these proteins had been solved, in the neuraminidase case at least. Researchers found out what the active side of that enzyme was, or the shape of that active sight. So they looked for molecules, small organic molecules, that drug companies could make and screened them and looked at whether these could fit into that groove of the active site of the enzyme and block it that way. So this can be a very rational approach for drug design.
Would these be fusion inhibitors?
Exactly, that might be one of the goals or might be one of the possibilities here. So there are no fusion inhibitor drugs so far on the market and not even in trial states for influenza. Although there are some in clinical trials for HIV fusion inhibitors, or entry inhibitors as they are sometimes called. So I talked about these large shaped changes in the hemagglutinin as it goes from PH7 to PH5 and opens the membrane that way. So if one could find drugs that could prevent that shape change from happening that would be a new avenue for new drugs. That’s one possibility.
Would that be like a preventative flu vaccine? Or would this be more of a treatment of really?
Basically it would be a treatment, and not a preventive drug.
So that’s a few years down the road?
That’s a few years down the road, as it is for basically all viruses. Fusion inhibitors or entry inhibitors have been found in HIV but they are still in clinical trials even there.
How does the World Health Organization decide what new drugs to come up with or what strains to target?
Well for making new vaccines, they get together at the end of the last flu season, say around March or so. They collect lots of samples from different populations all around the world and try to find out what their antigenic composition is, and then they make sort of re-assorted viruses from that in the laboratory. Then they grow large amounts of these viruses, actually in chicken eggs. These viruses are then harvested from those eggs and inactivated. This is what we get as flu shots. So it’s basically a dead virus that has been grown over the summer period in that way.
But we were saying it’s still sort of an educated guess as to what’s going to be on the horizon in the coming years. There is still a little bit of guesswork going on here too?
Yes. Yes, that’s true but I think the guesswork is usually quite good. I mean, people have done this now for many years and you know the flu protection vaccines that we get are pretty good. I mean nothing is 100% tight, or safe, but I don’t know what the current estimates are, what doctors would say. But I think that large numbers of flu cases can be prevented by administration of these flu shots. So that must mean the cases or vaccines that they made over the summer before that flu season must have been pretty good.
What are some of the challenges for you ahead? What are some of the big questions you are trying to answer here in your lab?
One thing that I would like to say is the research that we do with influenza virus here probably applies to other viruses, we know that many of these structural changes are in detail perhaps different, but in an accurate way very similar in different viruses. So we can learn about the influenza virus where the field is most advanced as far as the structural biology of the entry is concerned, and we believe we can learn a lot from this paradigm of influenza virus about many other viruses. We have recently gotten additional money from the NIH to apply some of our own methods to the HIV problem. We believe that with these methods we could probably learn more about the HIV and then you know hopefully improve those entry inhibitors that way. So our questions are, how are these shape changes and these surface molecules, HA in the case of influenza, and GP120 in the case of HIV, coupled into the membrane? What do these parts that insert into the membrane do to the membrane to suddenly change the membrane’s shape mainly to connect with the virus membrane and make a fusion core? So these are sort of the questions we would like to answer. Again can we find an inhibitor or a drug that could intervene at that stage? That is sort of the tools, or at the handles of these tools, if we could sort of change the shape of those drill bits so to speak, so that they would not fit exactly anymore into the membranes, the same way as they do in a natural case, then we would have also possibly a way of preventing infection from happening.
So what are you doing in this lab and what are the tools you are using?
So we are basically a structural biology lab using what we call biophysical methods to look at these processes. In our lab, we are using mostly spectroscopic techniques. So spectroscopy means you irradiate your samples with light, for example in the visible or infrared, even with radiofrequency. And you look at what kind of signal you get when it comes out again off the sample. If we interpret those signal changes correctly we can learn something about these shape changes both of the protein and the membranes. So specifically what we are using in our lab is laser fluorescent microscopy. So, that tells us something about how these membranes rearrange upon fusion. We are even in the process now of building the next generation of these laser fluorescent microscopes. We hope to follow this process on the basis of single molecules, so that we could detect single molecules, maybe HA molecules doing their job. Another technique that we are using is infrared spectroscopy. Yet another technique is NMR spectroscopy. And NMR stands for nuclear magnetic resonance. That is the very same principle that is used in MRI scanners to scan your body. You can use these same techniques also to look at tiny shape changes in molecules. And as a matter of fact, the noble prize in chemistry this year was just awarded, or half of it was awarded to a man who basically invented this technique for structural determination of biological molecules. And so we are using that technique in our laboratory also. Basically, what you do, you put your samples in large magnetic fields and irradiate the sample with a radio frequency, radio waves, and from those signals as I said before you can calculate back what your structure is.
Just amazing. So, these HA molecules they are so important. They are prominent targets for antibodies, is that right?
That’s absolutely correct. HA molecules are very important on these virus surfaces because they constitute about 80% of the total protein mass that is on the surface and that is actually exposed to the environment. So what antibodies in the circulation of our bodies see is mostly HA molecules, that is all they see of the virus, 80%. Maybe 15% or 20% is neuraminidase, so these are two major molecules. All the inner molecules and the inner nuclear capsid proteins of the virus are not really exposed to the surface. So they are not that important for the immune response in our body.
So what happens if these HA molecules mutate? What does that do to our immune system?
So when these HA molecules mutate they change their surface loops or some of their amino acids that are exposed to the surface. That will elicit a different set of antibodies in our bodies. So if we were, say, immune to a certain strain of, or a certain variant of influenza, then we would have antibodies against that particular HA surface or NA surface. But if they get mutated and change surface loops we would make different antibodies to fight those viruses.